IM Doc pt 38
Jan. 11th, 2023 05:10 pmSo, starting with June 2022... it turns out he was quite busy.
Without further ado...
Notes from the Deathcare world:
A relative was telling me how she just found out medicare would no longer cover podiatrist visits by diabetic patients. The nurse said it’s the insurance companies making the decisions. Not even the alleged “medicare supplement” is covering that procedure.
flora Is that traditional Medicare with medigap or is it Medicare Advantage (MA) that’s stopped covering? Medicare Advantage is not traditional Medicare. ( MA insurance companies go to long lengths to hide the fact their plans aren’t traditional Medicare or Medigap plans. surprise.)
IM Doc Your nurse relative has informed you correctly.
I just found this out last week when I had to admit an elderly patient for osteomyelitis of the toe. I was horrified to learn they had not had a podiatry appointment for some time. It is not that they are not covered – it has to do with how many they have in a year, etc. I just cannot keep up with the regulations anymore. Standard Medicare has one approach and then the infinite numbers of Medicare advantage plans have all their own. I often joke that they each get together and change the plan coverage every Tuesday afternoon. There is no primary care physician or office staff on this planet that can keep up with all of this. It is absolutely overwhelming.
To add on to the nightmare, there are dozens of my patients every day now playing “dial for drugs” because there are so many shortages everywhere. The above patient could not secure antibiotics prescribed by an urgent care and did not want to “bother” my office during COVID. Yes, we are now officially sending our elders out with prescriptions that may or may not be able to be filled.
If you have elders or infirm in your sphere of influence, I urge every one of you to keep an eagle eye on them. Things are already screwed up – and getting more screwy by the week. Many of them just do not have the mental acumen or the stamina to keep up with it.
I cannot stress enough – I have never seen this level of chaos in medicine in my life. Not even close.
It is not just baby formula, folks.
flora Thank you for this information. yikes!
ambrit Oh boy. I had better start seriously investigating “natural” substitutes for my hypertension meds.
Anecdotally, I still cannot find a medico around here who will write a prescription for “The ‘I’ Drug.” If anything, the local low socio-economic status clinic is visibly cutting back on procedures and scrips. My medica recently had a claim to Medicare for blood work related to my cholesterol level denied because it was “…too soon after the last claim.” (Her words.)IM Doc FYI –
This is a report from 60 Minutes from just the past few weeks about the issues related to drug shortages –
https://www.cbsnews.com/news/generic-drugs-pharmaceutical-companies-60-minutes-2022-05-22/
This report mainly deals with all the trouble that hospitals are having procuring simple basic drugs – like GLUCOSE – you read that right – GLUCOSE. We can make sugar galore for Froot Loops, Snickers, Dr Pepper and Hostess Twinkies – but making sugar for preemies? TOO HARD AND NOT ENOUGH PROFIT IN IT. What is happening to this country?
But the problems in the outpatient world are just as bad. Just now in the office a patient’s daughter reported the grandson had to drive 80 miles to get her mother’s potassium prescription. We had similar issues with magnesium this morning. Thyroid replacement is a very precise dosing – yet we often have to get by with higher or lower because many of the myriad doses are not available that week.
Getting things like Ensure and Boost for the malnourished is becoming an ongoing daily problem. Simple old antibiotics are often unavailable forcing us to use others that may not work as well or have unwarranted toxicity issues. Various types of birth control pills are up and down on availability and changing them out is not a great idea. And the shortages are rotating and unpredictable. What may be available today is impossible to find 2 weeks from now and then widely available again 2 weeks later.It really is all getting to be too much. I go into work every day telling myself – “I am not going to let anyone die today.” Simple things that we used to be able to do like personal call backs on labs and tests are just no longer able to be done. We have far too many critical issues that must be dealt with immediately. And there is the constant spectre of something falling through the cracks. That is not a sustainable morale. My staff, what we are able to keep employed, is just bug-eyed by the end of the day. I know from colleagues that this is more widespread than we would like to imagine.
I am not griping. It is an untold privilege to do what I do. But every day is a gut punch. And patients rightfully are getting more frustrated and angry by the day. I pray that what happened in Tulsa yesterday will not become the norm.
Space Station 11
My .02 regarding the current Covid wave…I too have heard of many in my circles testing positive, but almost exclusively with minor symptoms (including my elderly mother who was laid up for about 36 hours, but did take paxlovid). As for a community perspective, well, I am a mid-career emergency medicine physician at a larger inner city academic institution- level 1 trauma/burns, regional referral for ECMO- and I have not seen a ‘sick’ case of Covid in months. Probably not since 2021. By sick I mean- needing to be admitted on oxygen, needing to be intubated, considered for ECMO, etc. I’ve canvassed a lot of my faculty about this and everyone has the same experience- lots of positive tests, but usually with minor symptoms or completely unexpected (e.g. in trauma transfer patients).
I’m not sure what to make of this. I guess I have a middle-of-the-road attitude w/r/t the pandemic: I was very worried initially, treated a lot of very sick patients in the initial and Delta waves, I’m vaccinated and boosted (required for employment, although we had almost nobody in our staff quit d/t the vaccine mandate), follow masking guidelines when required but I will admit that I don’t often wear them in public now. Covid has become, basically, a nuisance to me- a reason for my kid’s daycare to shut down, as has happened multiple times requiring a very difficult scramble for my wife and I (she’s also an EM doc with irregular hours). Our entire family got Covid in January after my 1 year old brought it home from daycare, and there’s really no protection against that, which probably contributes to my current attitude. As for my patients, the opioid/meth crisis and a very obvious rise in violence (GSW/stabbings) over the past 1-2 years is a much bigger public health concern right now.
Just thought I’d give my thoughts as a long-time reader.
Fiery Hunt Thanks Doc…appreciate the perspective.
Been very much preoccupied by the conflicting thoughts of “This is an ongoing PANDEMIC!” and “It really doesn’t seem to be that big a deal…”
Nice to hear an informed voice that’s not screaming “We’re DOOMED!”
Fiery Hunt And just like that, Alameda County in SF Bay Area just reinstitued an indoor mask mandate today.
https://www.sfgate.com/bayarea/article/Bay-Area-county-mandates-masks-17215847.php
IM Doc I am not sure what to make of this whole situation either.
And it is always good to have other physicians with whom to compare notes.
The COVID pattern in the past 2 months has taken a completely different direction than I would have expected. I live/work in a very vaccinated area that is surrounded by very unvaccinated areas.
We are no longer doing any kind of official counts through the health department for outpatient care – so I have no official numbers. What I am seeing and it has now been a fairly consistent pattern for weeks is absolutely huge numbers of cases in my own practice – as in 7-8 times the numbers seen in the exact weeks from 2021. In a population that is now almost completely vaccinated. I find that very concerning. The same cannot be said of the unvaccinated areas which I really am not hearing from at all. So that right up front is a problem. We are having many times more the cases in a year that has vaccinated patients – compared to a year that did not – 2021. And almost entirely, the cases being called into me ( assume that would be the sicker patients) are from the highly vaccinated areas and almost always vaccinated/boosted patients.
Furthermore, seeing a routine around 5% of patients being routinely screened in the hospital prior to surgery, tests, etc being positive and having no symptoms at all. Just found on routine screening. This is a rather large number. Multiple issues as outpatients living in the same house where I have all the vaccinated/boosted patients ill, while the unvaxxed are positive but with just minimal symptoms or not sick at all. Very strange.
Seeing the exact same thing here as you are as far as admissions – almost zero. And the ones that are being admitted are often for social reasons – and would never have been dreamed to be admitted when the hospital was stressed. And certainly no ICU, vents, or ECMO.
But many of these patients as outpatients are indeed fairly ill – but not hospital level. Again, the concerning thing is the overwhelming preponderance of these ill patients being vaccinated/boosted – and the fact that they are in such much higher numbers than what was seen in early June 2021.
Since no formal numbers are being counted, it is very hard to make any judgements. But with talk in the doctors’ lounge it is clear my colleagues are seeing mostly the same thing. I am hearing similar stories from my colleagues across the country.
So we have a vaccine that seems to definitely be preventing death/bad illness, at least from acute respiratory issues. But at the same time, as outpatients, the vaccinated seem to be much more affected with case numbers and outpatient illness. Almost invariably, the sicker the patients are as outpatients, the more likely they are to have been vaccinated/boosted. Really vastly so. I do have concerns with this pattern going forward and what this may portend if more noxious variants are conceived.
I have never felt so strange as a physician. I have been trained and practiced for decades to take in what I am seeing around me and listen to my colleagues and mold what I do based on what I am seeing. But, those in charge of our public health apparatus seem intent on continuing on the same course and not really being too transparent with how they are arriving at their recommendations. It is very disquieting. Because a lot of what is being recommended does not seem to be appropriate with what is going on in my world or many of my colleagues.
I am not sure what to think. One thing I know for sure. This is not over.
Fiery Hunt One possible thought as to why the vaxxed are “sicker” than the unvaxxed:
Behavior.
Vaccination rates here in the Bay Area are pretty damn high and Alameda County just announced there’s more hospitalization now than last summer during Delta.
So many people here in the Bay Area act as if getting “boosted” is some sort of magic spell that wards off Covid. Travel, gatherings, hell, just going out to restaurants, bars, music venues..
Can’t help but wonder is there isn’t a correlation between wealth, lifestyle and being an extrovert…(high vaccination rates) vs working class (“essential workers”!) introverts…(non-vaxxed).Spending hours in gatherings, traveling, attending events versus just wanting to go home.
The alternative seems to point toward a vaccine= worse response to infection and that’s a whole nasty can of worms.
IM Doc https://www.cbsnews.com/news/covid-19-vaccine-boosters-infection-rate/
This is a classic example of what I am talking about. The article seems to be pointing out the same thing I and my colleagues are noticing as I describe above.
What is concerning to me is the response. My response would be “what is going on medically to produce such an outcome?… what if anything does this mean for the future?…..how should this help us with our advice for the legion of increasingly skeptical patients who are asking every day about getting a 4th shot?” The response described in the article is paraphrased as such – “recording case calculations is the problem, therefore, we should stop doing it.” No curiosity about why this is happening.
Understanding WHY things are happening is often a fundamental part of understanding biomedical issues. This is the beating heart of being a diagnostician. And so many times we seem to be ignoring the WHY because the numbers are inconvenient or not fitting the current narrative.
I can point to many many such articles where the discussed response does not seem to make much sense. This is what is being pushed out to our populace. They are not stupid. They see the same things I do and are bringing them to me daily unsolicited. It is very frustrating for everyone.
NC post says: IM Doc flipped out when he saw this tweet. And GM confirmed that it’s not true, that more died under Biden even if you give him a one-month grace period after he was sworn in:
Here's NC talking about hospitals gaming numbers (heh, that's only happening in June of 2022?)... and they have very nicely quoted the famous Dr. Natalia as well... When I clicked on her link the original post cannot be viewed (must be blowback from being ratioed) -- but also interesting to note that the follow-up comments are filled with people asking "Really? Is this common? Haven't seen that here?..." in other words, Dr. Natalia, cite your sources?
A new way for hospitals to game the data:
IM Doc writes: “I would guess with Omicron about 60% of the patients were on Dexamethasone – so no – not an adequate proxy” for hospitalization.
Just a reminder:
As with everything else, because the United States is not a serious country, our hospitalization data is bad. Here the baseilne is off:
Hospital trick: patients admitted with covid in 10-12 days become post-covid & no longer counted as hospitalized covid patients. ICU is full of post-covid patients that are here for 30, 40, 50 & more days. Not counted in the official stats.
— Dr. Natalia
(@SolNataMD) January 24, 2022

I thought Obamacare was going to be affordable? Remember it was called the Affordable Healthcare Act?
A plan put in place by the party of the working man, with a big smile on their face. “It is a big f#$%ing deal”.
Actually Obamacare was the final nail in the coffin of my profession. It was the hand-over of all that generations of physicians had held dear. Handed over with gusto to Big Hospital, Big Insurance and Big Pharma.
There are now more people in debt to these big industry companies than ever before. And they have no compassion, no mercy, no soul.
Every single month, when I have new students, one of the first things we do is listen to an old song by Woody Guthrie — the best rendition of it is by Merle Haggard at this link –
https://www.youtube.com/watch?v=e0f78MDOUJw
I reiterate the following words from that song to those students all the while they are looking at me as if I am from outer space ——
Jesus Christ was a man who traveled through the land
Hard working man and brave
He said to the rich, “Give your goods to the poor.”
So they laid Jesus Christ in his grave.
He went to the sick, he went to the poor,
And he went to the hungry and the lame;
Said that the poor would one day win this world,
And so they laid Jesus Christ in his grave.
Yes, if Jesus was to preach today like he preached in Galillee,
They would lay Jesus Christ in his grave.
American New Deal Liberalism at its finest – something that virtually no one remembers today in all our woke glory.
I know I am the old man from the before times. I realize that. We live in such a much more advanced world today, don’t you know.
For thirty years, I did everything I could to model this for my students and residents and colleagues. Just as it had been modeled to me by my grandfather. He gave everything he could to help those around him – and died not wealthy in financial terms, although not poor either. No, he died very wealthy indeed, as there were 6000 at his funeral praising him for all he did for them.
I do my best to tell these kids it is far better to build your obituary than it is to build your resume. There is something transcendental about giving everything you have and expecting nothing in return. It strengthens you to give your time and energy to those who have nothing.
My profession has sold its soul to Mammon. The consequences are just now being fully realized. My grandfather always told me about his youth. And how it was all fun and games until one day the money just vanished. “That will happen to your generation one day, son, and when it does you will know instantly who you can trust.” His words strengthen me every day as I see this going on all around me. I know it cannot last long.
I must get something off my chest.
There is also a lot of very incorrect information circulating about this issue and I feel it needs to be addressed so we can all be on the same page.
You may have heard that the American Board of Internal Medicine ( ABIM from now on ) has decided to go after Drs McCollough and Kory – 2 of the more famous dissenters from the COVID narrative. This all blew up over this weekend. I am hearing from all kinds of sources online that ABIM is going after their LICENSE.
Please note – this is NOT THE CASE. Licenses to practice medicine are administered by the states. The ABIM nor any other Board can go after someone’s license. They are however, trying to strip them of their ABIM certification. That is a way in which the ABIM certifies that a doctor has demonstrated expertise in whatever field it is given. These are completely separate issues. The ABIM is duty bound to report anything negative it finds about a physician or their conduct to the state licensing board, but that is the end all to their ability to affect a license.
Losing your Board Certification however is not without consequences. Most insurance companies will not contract with physicians unless they are certified. Most hospitals will not have them on their staff either. However, a physician can obtain a license from any state in the country and practice medicine.
The bureacratic overreach of these certifying boards has been the subject of much strum and drang the past 10 years or so. They are very expensive and time-consuming to maintain and have basically become a manner of rent extraction from the plebes to the medical elite. In my and many other’s opinion, the initial certification is of great import – all the rent extraction and multiple tests for the rest of one’s career does nothing but enrich the chosen few of these Board’s leadership. It is very much a scam. The entirety of this can be found documented for years on the following website – drwes.blogspot.com – if you are so interested. In recent times, this has led to multiple states banning the Boards from this onerous behavior.
Alas, the ABIM has now apparently dragged the AMA into this whole affair. The AMA has put out a very ominous statement in the past few days that they will be going after any and all spreaders of “disinformation” and will be using the social media, media, Medical Boards, State licensing agencies and anything else at their disposal to silence the evil doers.
As a medical historian and teacher of history for decades, I would suggest to the AMA and I have already personally relayed to the 2 members of the ABIM that I know personally that medicine has a very long history of exactly the kind of behavior they are planning. I am very hard pressed to come up with a single instance where it has worked out well for those going on the witch hunt. In fact, it has often detonated in a very bad way for them. I am going to assume this will end in a similar disaster for these agencies and they should take heed of the warning from history before they have completely torched whatever credibility they have left.
Medicine is science. And unfortunately, for these people who have decided science is their new God, it is never settled. Just in my career, I have seen aspirin, statins, hormone replecement therapy, and opioids used for years because it was “settled” science only to have that overturned with lots of experience and lots of very good research. I have also sat and listened to countless presentations and debates about these issues that were often very vehemently violent. Everyone watching knew the stakes, and knew the hearts of the partisans on both sides. But the verbal and public debate was critical for our understanding and how to proceed going forward. Those who have their finger on the scales thinking they “know the way” are often proved very very wrong.
So censoring or punishing these COVID dissenters in a very public way like this is exactly the wrong thing to be doing. These agencies seem to have no clue that they are holding on to just a shred of credibility that could vanish if they are perceived by the public in the wrong way. A much more appropriate way to handle this is to get McCollough and Kory on one side and experts of your choice on the other – and let them have it out online or on national TV. Everyone in this country has a stake in this debate – let the American people watch. Dr. Hotez and Dr Offitt and Dr. Wen, there will not be a better way to make these two like boobs. You are clearly very confident in your position – I would say go for it. WHAT DO YOU HAVE TO BE AFRAID OF?
There as so many examples of this behavior in medical history that have gone off the rails for the witch hunters, it is hard to come up with a “best” one. Probably, the most congruent for a situation today is the case of Dr. Ignasz Semmelweis. I would encourage everyone to read his story. It is so important that the pre-eminent medical historian of the 20th century, Sherwin Nuland, wrote an entire book about him called THE DOCTOR’S PLAGUE.
Dr. Semmelweis had an idea that he felt would make life much safer for patients in the hospital He went all over Europe and discussed his findings in all kinds of venues. The areas that followed his advice, notably Scotland and parts of France, had marked improvement in the situation. That did not sit well the leaders of the day – most notably Dr. Koch ( famous for his postulates and the Fauci of his day). He and others went about destroying not his ideas – but his reputation, his livelihood and eventually his sanity. They did not really want to argue the merits with him – just tarnish him.
What was the grave “disinformation” that Dr. Semmelweis was peddling? It is basically local infection control in the operating room , ie the aggressive use of PPE and disinfectants on the skin during surgery. This egregious “disinformation” has likely saved billions of lives since Dr. Semmelweis.
A Supreme Court justice had a famous line that “sunshine is the best disinfectant.” Jesus Christ himself taught us that we will know the truth, and it will set us free.
ABIM and the AMA – I urge you to get these two on the stage and let’s have a real debate about these issues. If your contentions are so correct, what do you have to lose? Give them everything you have – make them look like morons…….WHAT ARE YOU AFRAID OF?
My concern is they saw the Dr. Fauci/ Rand Paul exchange last week and realize there is actually a lot to be afraid of.
voislav McCullough has repeatedly lied about vaccine sideeffects, including claiming 50,000 deaths from vaccines in the US. He didn’t do this as a private citizen, he used (and misrepresented) his medical credentials to advance this information. I’ve done tons of scientific research (50+ papers), worked on covid research early in the pandemic, so I am familiar with how bad a lot of covid research is. That is not an excuse to go about spreading lies, lies that cost lives.
When it comes to McCullough and people like him, I take a very dim view. Criminal charges should be a minimum, forget revoking their medical license. I understand the argument for open discussion, but not when people are dying because of their scummy behavior. There is no reasoned discussion when one side is making stuff up. Show me data, we can discuss how dismal statistical analysis in medical sciences is, but the onus can’t be on one side to disprove assertions made without any evidence.
IM Doc There are times in emergencies when we as practicing physicians have to not depend so much on exact studies which will come much later. We have to depend on what we are seeing and hearing with our own eyes and pay very close attention to colleagues both in our area and those we know elsewhere.
So what have I seen with my own ears and eyes? I have one patient in my practice who most certainly died from the vaccine complication. I have done all I can do to report it last April and was completely blown off by both the FDA and CDC VAERS program. Interestingly, it is a very unusual problem that was the demise of this patient that timed perfectly when they got the vaccine. Over the months, this problem has now become a fairly commonly reported issue with these vaccines. I have also had two other patients who just literally dropped dead within hours/days of the vaccine. Both were younger and healthy at baseline. I cannot as safely call them vaccine deaths. It may have been random chance but I doubt it. I have had another patient who had the worst blood clot I have personally ever seen within days of the fourth shot and died from it. I have had 27 severe or critical vaccine complications over the past 18 months, confirmed to me just today by an audit of charts done by colleagues in my hospital noting how much higher this was in 2021 compared to the past two years.
This is real time information. It will not appear in any published studies for probably years. It is definitely a clue to what has been going on, though. And we cannot ignore the most ominous issue which is the very substantial increase the life insurance companies are having to pay out since the introduction of the vaccines. I am certainly glad that you have read 50 plus papers, but my life’s training and work would say this kind of data will arrive in papers much later. We must react to what is going on now. On the ground docs must monitor all that is going on around them and make judgements.
I have many colleagues all over the USA who will readily admit that yes they have had at least one vaccine related complication leading to death. It is not uncommon at all. Unfortunately as you state no one on a federal level is too interested in improving data collection.
A quick Google search reveals there are right at 65000 practicing internists. Let’s say a third can make the 1 death statement. I think that is probably low from discussions. That would be 25000 deaths or thereabouts. Now, we must add the even larger workforce of family and general practitioners who number over 100000 and all of a sudden the 50000 number is not out of the ball park at all.
I can see where a reasonable person could make that claim. And I would be willing to testify to that in court and even bring these patient’s families if needed and let the jury decide if the timing of the deaths and their nature are realistic for vaccine issues. It may come to that since the FDA does not seem to be really interested in helping us with this issue at all.
And sorry, your claim of scaring people holds no merit. Look at the rotavirus vaccine disaster of 1999. I believe we had less than 20 deaths from that and it was suspended instantly. The swine flu disaster was less than 50 patients. The denguevax did not even make it out of trials because of this issue. There was a time when we weighed risks and benefits and realized that even 20 or 50 deaths across the country was too high a price to pay. Surely, you must realize there have been way more than 50 deaths from these COVID vaccines. But now Pharma has co-opted our regulatory agencies. We are the blind leading the blind.
I think there’s a larger game in play here.
You’re right that the most rational and fair way of addressing the dissenters’ views is a public debate. However, that lets the dissenters speak, and the real point is to prevent them from speaking. The method chosen by the elite also discourages future dissenters from getting ideas–my guess is that revocation of board certification (which, as you note, already has serious professional consequences) is just a way point towards the real destination of onerous state licensing investigation and (in the establishment’s ideal world) license revocation.
It’s all just another variation on “lawfare.”
To that end, Drs McCollough and Kory are ideal targets. Both were pretty successful physicians if you look them up.
IM Doc Both are so successful as physicians that it is going to be very difficult to take them down using this tactic. If they succeed in gutting their ABIM certifications, I can guarantee you that the lawyers will be lining up to take their case. I happen to know two of these lawyers who take on Medical Boards and licensing agencies on the behalf of physicians and their nicknames among their peers are Ballbuster and Nutcracker. And they have earned every bit of those names..
I have read the list of wrong think put forth by ABIM on both physicians. If they do take away their board certification, lawsuits will soon follow. And then in the course of events will be discovery. I know enough about the situation to realize that if discovery proceeds, I am thinking the ABIM may be in a very bad position. Especially in this climate of every month something new comes out. For example, a year ago, both were being cited for discrediting the claim of 98% effectiveness and that the vaccines would cause the vaccinee to be a dead end for transmission. How has that worked out in the fullness of time? There are other things on these lists that I am certain will be just as likely to not go well for the establishment narrative.
In other words, this has the potential to be very interesting. Stay tuned.
Sorry, this was meant for the censoring article……this is in regard to the impending investigation of COVID narrative challengers Drs. McCollough and Kory. Sorry all, I put this comment in the wrong post……..
And for those interested in how the ABIM ( American Board of Internal Medicine ) conducts their investigations, I would point you to this piece of journalism.
http://drwes.blogspot.com/2017/03/fact-check-on-abims-director-of.html
This was a few years before COVID, but as far as I know, the basic regime is still in place. These organizations are accountable to no one, certainly not their members.
Please note, it is not physician scientists who are investigating, it is washed up GI Joe military-adjacent goons with an attitude. I can only imagine how their “security” thinking has evolved since the start of this pandemic. Sadly, my forebears in medicine would be shaking their heads in absolute shame.
America, is this how you want this COVID issue investigated? This approach or a public debate?
This is all very concerning to me. The health of the nation is involved here. Why are not enterprising young journalists not all over this stuff? This is what careers are made of.
flora Thanks for the link. I’d guess if the ABIM pulls their board certification of either of these two docs a lawsuit will follow, where discovery should be interesting.
Tom Stone There are perhaps three internet based outlets where an enterprising young journalist might get such an expose printed.
None of the networks would touch it and none of the print outlets would either, with the possible exception of “Teen Vogue”.
The going has gotten very weird indeed.IM Doc I can answer my own question about the young journalists.
Here is today’s wonderful example –
https://twitter.com/mtracey/status/1539086445209690112
One of the most well known reporters at The Washington Post mocking and condescending a suffering COVID patient.
Lateral ableism???? In decades of human care, I have never heard that expression even once. When I performed a google search, there were three different definitions, and for the life of me, I cannot figure out how any of those definitions applies here.
These people just like to throw out “big words” and hope that everyone thinks they are really intelligent.
I used to think that this young reporter, Ms. Lorenz, had all the signs of narcissitic bipolar syndrome with a touch of borderline. It is becoming more and more clear to me by the day that she would fit right in with Ti or Do of the Heaven’s Gate Cult.
Of course the Washington Post of Watergate lore is not investigating any of these important medical things now – they are too busy giving this psych patient a platform.
I don’t think she was mocking him (that was the whole point!), but she was certainly atrociously condescending. She was also stupid to call out Yglesias for his original joke. I mean, pick your battles, Taylor.
A real shame because as far as I can tell she is one of the few mainstream journalists who continues to draw attention to the ongoing seriousness of SARS2 and Long Covid, which is a genuine service at this point. Unfortunately dragging out stupid shite like “lateral ableism” instead of something like “yep, you know what, fair play, I see your point, good health to you” is not exactly ‘hearts and minds’ stuff.
I must admit, as a psych patient, I am surprised to see you refer to psych patients with such casual derision. Presumably people with psychiatric illness are entitled to journalistic careers, so long as they don’t go full Stephen Glass?
IM Doc Yes – even I get carried away with my disdain for these people. I should be much more measured with my words.
What I would say is she is the toughest kind of psychiatric problem to deal with. She has a severe personality disorder. Probably borderline given her behavior when I have seen her on TV interviews and her propensity to dox and torment people for doing the same things she is. Projection is one of the worst symptoms of borderline and she seems to have added severe passive aggressive tendencies. She is also very adept at what is known as “splitting”. That is a well known combo for a very difficult and frustrating patient. They cause nothing but chaos among providers when we try to care for them. We physicians use the words “psych patient” and quite frankly worse frequently to vent our frustration in private to peers and really that has nothing to do with the legion of people out there who have organic psychiatric issues like depression anxiety and schizophrenia, etc.
It is very concerning to see someone with this type of behavior being given such a platform where she can manipulate and “split” an entire country.
Again, I should be much more measured with my words and realize I am not with peers on this board. For that I apologize.
Unfortunately as is so often true with borderline patients, any good in the world they do is often extremely overshadowed by all the antics and mayhem they cause – just like this reporter.
So Doc, remember back when I had some harsh things to say about Alex Berenson, among others? You made a rather impassioned argument involving the need to accept that bad people can do good things, even if for the wrong reasons.
Taylor Lorenz has, as Basil Pesto notes, been a rare mainstream media voice calling for Long Covid to be taken seriously. Yglesias on the other hand is a minimizer.
Who cares what sort of emotional horror show Lorenz may be?
Additionally, while I greatly appreciate your contributions here, and I’m deeply grateful and indebted, to you for them, your remarks about Lorenz seem perilously close to tele-diagnosis. And surely your last sentence isn’t meant to imply being a psych patient should make one subject to deplatforming*? But it reads that way – what exactly is her offense?
*If it does mean that, can we deplatform that Canadian loon psychologist? I’m against censorship, but I’m really sick of his face showing up in my YouTube suggestions, and the republic’s shot to hell anyway, so ill wind and all that …
IM Doc Well, psychiatry is the one area of medicine that is very able to be characterized on video and what someone wrote. Indeed, 2 of the 4 semesters of my med school human behavior had finals with just 10 written paragraphs and we had to identify the psych disorder from the written word. 1 other semester had 30-60 second snips from movie and TV shows of behavior that we then had to diagnose and the other semester had brief live acting.
It is fairly easy to identify personality and behavior disorders from video snippets. Her videos I would say are classic textbook examples of behavior identified as borderline and narcissist. I would be happy to use them in any demonstration for students when trying to demonstrate it. I do this all the time. Just today, I used a short snippet of Sophia from The Golden Girls to demonstrate to my students confabulation – a sure sign of micro vascular dementia.
As for why she got all my animus about that tweet. I have zero tolerance for using photos of suffering patients to make any point. Especially a virtue signaling point. For the same reason, I had such vitriol for all the young doctors making TikTok videos about the unvaxxed. If I had exhibited either of those behaviors as a medical student or resident 30 years ago, I would have been fired instantly. I would flunk a student on the spot for the whole rotation if they pulled a stunt like that just once. We live in a different world now but I tend to not just ignore but actively dismiss anything people who use these tactics say. I find it incongruent with informed discourse.
I would appreciate if you could point me any place that Berenson has taken a photo of a suffering patient and behaved that way. I certainly have not seen it. He is often very juvenile in his comments but nothing that rises to the examples I have outlined above. Indeed, his juvenile comments often make what he has to say very difficult to get to. But again, I have never seen him engage pictures of suffering people. I have a tolerance for him because he is one of the few journalists that truly seems to be able to handle statistics in medicine. He had the Big Pharma beat at the NYT in the day they when were doing real news. You can instantly tell the difference between him and the stenographers that are all over the mainstream media today covering this story. He is the only one I know of that understands relative vs absolute risk, as one example, and did his best to explain that to people all the while the NYT and CNN were screaming 95% 95% 95%. I realized long ago that Berenson is an example of how the media would have handled this pandemic in my youth – tough questions and hard nosed assertions. It was amazing watching as all the other media types melted like snowflakes in reaction to him this past year. And because he actually knows how to engage scientific literature, who has had the benefit of being proven correct way more often than these others? As a professor, we learn to put up with a lot from students when they are being hammered by others but who clearly are persistent with their convictions.
About her take on Long COVID. This may be so. But what is happening to her is one more piece of evidence I have that she is deeply into borderline personality. It is a characteristic of these people that whatever good they do is dwarfed by their constant antics and hysteria. A comment above points out she has been demoted. This too is characteristic. Constant job loss, resignation or firing. People cannot stand to be around them as charming as they may be. If she is the spokesman for Long COVID in the mainstream media, I would suggest that position needs someone else immediately.
By the time they are 50 or so most of these borderline patients have had it hammered out of them. If they manage to survive. I certainly hope she can see that while being demoted and begin to work on her behavior.
Raymond Sim Well, psychiatry is the one area of medicine that is very able to be characterized on video and what someone wrote. Indeed, 2 of the 4 semesters of my med school human behavior had finals with just 10 written paragraphs and we had to identify the psych disorder from the written word. 1 other semester had 30-60 second snips from movie and TV shows of behavior that we then had to diagnose and the other semester had brief live acting.
Wow, your response is far more interesting to me than the original topic, and coming from you it’s quite disconcerting.
Eschewing all sarcasm, your remarks strike me as an indictment of psychiatric diagnosis, and potentially medical diagnosis and pedagogy generally.
Is it just me? I’d be very interested to read others’ takes on the passage I’ve quoted.
IM Doc Actually I would disagree with you.
I would make it very clear that the teaching of human behavior in the modern medical system is just a remnant of what it was when I was young.
My education in human behavior came from a line of thought back then that was called “transactional analysis” – I’m OK – You’re OK. It was about half the time in the first 2 years of med school – that is how important it was thought to be for medical providers.
TA was very big in the 60s 70s and 80s. Not so much now. I do think it should be though. I see students struggling with dealing with patients all the time.
Basically, it employed what is known as the therapeutic sequence. To make things simple – there are about 15-20 different personality types. And you as a provider should be able to spot them instantly. They all behave in very different ways. And not just active behavior – how they hold themselves, how they dress, how they do makeup, how they speak, how they move their eyes, hand gesticulations, how they move their mouths, etc.
About 40% of the population is estimated to be what is called “a genital character” – you are able to bounce around in the personalities depending on the situation. Sometimes, it is important to be antisocial sometimes histrionic. These patients are considered “normal”. The other 60% are “stuck” in one of the personalities and are dysfunctional because of it.
And you as the provider have to be able to recognize these instantly, because how you proceed through the therapeutic sequence is dependent on what you are seeing from them.Therefore, it is critical to be able to instantly evaluate appearance, cues, speech patterns, eye movements, mouth movements, etc. You must know the “character” you are dealing with at all times. You would approach telling a borderline they have cancer much differently than a schizoaffective, etc.
It takes years to master this – but it is essential. And it is a large part of what makes a “bedside manner.” But this type of thing is completely ignored in modern medicine – these kids today are learning none of this.
Accomplished actors know these things instinctively and can change their mannerisms accordingly. For example, within 5 seconds of seeing Glenn Close in Fatal Attraction, I knew the character was a borderline personality disorder. She is an incredible actress. And yet within seconds of watching Glenn Close in Dangerous Liasions it is crystal clear that her character was a narcissitic personality disorder.
Within seconds of watching or listening to Stevie Nicks, it is crystal clear she is a schizoaffective personality – and the witch stuff all makes sense. I can go on and on and on. And as a physician, I would handle these patients very very differently.I am very appreciate of the era in which I grew up. Human behavior and the ongoing mastery of it is essential for a physician – and it is being completely ignored today.
On the topic of COVID, Eric Topol commented that BA.4 and BA.5 (taken together) now represent 35% of new cases in the United States:
https://twitter.com/EricTopol/status/1539267655604924417
He also mentions the new study on the risk of reinfection. Deepti Gurdasani has a thread about that:
Basil Pesto The reinfection study is ‘hoo boy’ stuff. I expect it will be hoisted to links tomorrow. The general conclusions aren’t unexpected by any means but to see it so starkly in writing is… rather bleak.
psmith Yes, I found it upsetting reading, especially in the context of precautions being dropped and new variants becoming dominant.
IM Doc This is an example of something I am seeing on the ground. In rather large concerning numbers. Lots of reinfections and many are so quick after the preceding infection. This is a first blush attempt at research for what me and many colleagues are already seeing for the past month or so since the post-Omicron phase started.
It seems like the patients tend to get more ill on every episode as well.
I really would like for someone to really do these kinds of studies with the vaccines in mind. They do not appear to be effective in stopping this at all nor do they seem to be that effective in mitigating the symptoms. What is very concerning to me is to this day is that many of the vaccinated have a feeling they are safe and sound. If they get sick, it will not be bad. They CANNOT become critically ill. So far we are not seeing that much critical illness – but I promise you, the vaccinated are getting very sick.
I am really concerned if/when a more virulent variant comes around.
Here is IM Doc's comment following the post:
I view my most important job as a physician to be education of my patients. To tell the truth as I see it at all times and to give my commentary on the current data based on experience. I took to doing this on this site earlier in this pandemic because I could not see that was happening too often in the media landscape.
As such, I will give this update on where we are in my practice with just today’s numbers, which I will be discussing with inquiring patients today.
My staff and I maintain a spreadsheet daily of what we are seeing. No one in officialdom seems to care about this type of on the ground data – but I think one day it will be very helpful for those learning about what happened during this pandemic. Every morning I am given a condensed top line list of the patients with COVID that were encountered the day before.
Right up front, I work in one of the most vaccinated counties in the USA, >80% vaccinated – >60% boosted. The surrounding areas where a good number of my patients come from is at best 50% vaccinated.
Yesterday, I had 45 COVID patients evaluated by me or my staff. More than 50% of these were from 2 different superspreading events, one a wedding, the other a performance. Out of these 45 patients, one was completely unvaccinated, 17 were double vaccinated, 9 were vaxxed with one booster and 19 were vaccinated with 2 boosters.
The very concerning thing to me is how many of these were reinfections. Of the 45 patients, 37 were reinfections, and 11 of those have just been within the last 6 weeks.
This is right in line with what I have been seeing for the past few weeks and it is also right in line with what is reported in this paper. Reinfections are becoming more and more frequent – and the patients, vaccinated or not, are getting sicker with each episode.
First of all, the majority of these patients at this moment in time are not all that sick. But some of them really are quite ill. 12 from yesterday to be exact.
Much has been made of Simpson’s paradox in our national media the past few weeks in an attempt to explain away all these infections and reinfections in the vaccinated. It is a very complicated statistical concept, but in general it basically is this – I work in a >80% vaccinated area so I would expect >80% vaccinated patients. Therefore, we are good. THIS IS EXPECTED. The writers of these articles know nothing of medical statistics and this is profoundly misleading. It is making people much more comfortable than they really need to be.
It is absurd to invoke Simpson’s paradox in this situation for 2 reasons –
a) Simpson’s paradox has never been invoked in a vaccine situation to my knowledge – not one time. This goes back to the sterilizing vs non-sterilizing issue. We would just not even see patients at all if the vaxxes were sterilizing. Simpson’s paradox is perfectly appropriate to discuss in medical therapy for heart disease, etc.. For vaccines, it is completely inappropriate.
b) Much more important – June 21st of 2021 – I had 2 COVID patients – in a much less vaccinated environment – June 21st of 2022 I had 45. This is important if you assume some seasonal variation. YOU SIMPLY CANNOT HAVE THIS LEVEL OF DIFFERENCE and invoke Simpson’s paradox
What these writers and news outlets are doing is very dangerous – and is giving the vaccinated a sense that they are bulletproof. WE ARE ALL GOOD – MEDICAL STATISTICS TELL US THIS WAS EXPECTED – EVERYTHING IS GREAT. This is not a good message. It is not based in reality.
My education bullet points to my patients—— This is very serious. Your vaccine status is giving you zero protection from catching and transmitting this virus. We have no idea what these frequent infections can do to you, but my sense is it is not good for you. PLEASE PLEASE do not depend on this vaccine to protect you from infection. Take every precaution you can. There is evidence that it may protect you from severe illness, but even that seems to be not as solid as it was before.
And I go back to what I have been saying all along. Get healthy, get your a1c down, get your waist size down. Eat well. Sleep well. Enjoy good times with your family. Get out in the sun. De-stress. Get going on the VIT D and ZINC. Please please be careful.
Everyone here – I would say the same to you – please be careful.
.....
I will, however post the entirety of this next post as it's pretty much IM Doc's email to the NC folks:
Growing Revolt Among Medical Practitioners Against Vaccinating Toddlers for Covid
IM Doc has been particularly unhappy about the push to deploy the Covid mRNA vaccines in children under five years of age. Based on his many years working on an Institutional Review Board, he believe the bar for safety testing for children, particularly very young ones, is high, and it has not been met for these vaccines.
It turns out he is far from alone. It appears many medical practitioners are seeing vaccinating kids this young as a bridge too far and some are flat out refusing to administer them.
From IM Doc via e-mail:
I had a moment today where I realized that it may very well be the nursing and the pharmacy professions that begin the long slow pushback against the overprescription of Covid vaccines.
Two things in two different parts of the country happened.
Today in our county, which recall is over 80% vaccinated and hence has been very receptive of Covid vaccines for adults, I was called to an urgent meeting because it may be that hospital staff would need to be pulled to the Health Dept. Why? – Because the inoculation of the less than 5 is beginning – and all 3 of the Health Department nurses resigned in protest. They are simply not going to give these kids these inoculations. When a nurse on my staff was approached with filling in the deficit – her response (in my presence and that of the supervisor) – “Not only no – but FUCK no.”
It turns out the county Health Department found no nurses willing to do this. So our entire vaccine program for everyone not just kids was on hold.
After more panicked efforts, they found one nurse to give the shots. That nurse too refuses to give it to the babies. She will be there only to do the shots for 18 and up. She will not even give to teens. I am sure they will eventually find people to do it, but it is profoundly admirable of these nurses. I will be doing all I can to help them get other employment.
I had asked if the county Health Department would try to get the three nurses who had resigned to return, now that they had relented and were letting a nurse administer the Covid shots only to adults. His response:
I am pretty sure they would welcome the three back with open arms. But they will not go back because they are just not going to give to kids. I have talked to one of them this evening. As is so common in medicine and nursing now, moral injury is at play. They have put up with so much, this was just a bridge too far. They hired this other nurse in an emergency situation to make sure the place was open. They will find others in the next few days, I am sure. Although finding nurses for anything is very difficult right now. It is just the loss of seasoned employees is not good. And it will cause some chaos if they have to be pull nurses from other jobs.
Additionally, my sister has now informed me that at her health dept in a distant state, one of their nurses have refused to give to under 5. They are not fired or resigned but it has really caused an enormous delay in appointments.
Physicians are hearing that the pharmacists in the entire Publix chain of grocery stores in the SE USA were in such an uproar about it, that Publix will not be offering these vaccines to under 5 kids. The Tampa Bay Times confirmed that Publix won’t give the Covid jab to kids below 5. Good on them.
The “pharmacists refusing” isn’t yet reported the press, but I did track it down with my cousin, a Publix pharmacist in VA. He confirmed the story. Lots of pharmacy pushback because a) many do not want to give it to babies b) many do not feel adequately trained to give to babies. My cousin feels fine giving to toddlers but he too feels about as conflicted as I do that the data does not support it. “I would not give any other drug with no evidence special treatment……why should this vaccine be any different”….
Similarly, in the infectious disease conference yesterday AM (a regular and large Zoom meeting of doctors affiliated with a major teaching hospital), this topic came up. The retired infectious disease doc that has been one of my heroes stood up and had a single slide:
There have been 350 deaths of under 18 with COVID since the beginning of this pandemic – and we know that at a minimum more than half those kids died with COVID not from COVID. 350.
And when I did a VAERS search yesterday – for patients aged 0-17 – 0-3 days post inoculation this is what I found:
Death and Permanent Disability
J&J 1
Moderna 37
Pfizer 237
Total 275Hospital Admissions or ER visits
J&J 13
Moderna 266
Pfizer 5527
Total 5806So in the same time we have had a mere 350 (and probably more like half that number) of kids die from COVID – we have killed at least 275 with the vaccines, and sent 5806 to hospital or ER…….And this is moral? This is ethical? Can someone please explain to e how this is not a violation of the Nuremberg Code?
I can readily tell from my interactions with other large academic Zoom conferences and also multiple consults with tertiary docs the past few weeks that the worm is turning. The injuries these things are causing are just no longer going to be hidden. AND WE ARE DOING THIS TO TODDLERS.
I personally looked over the 37 Moderna deaths today on VAERS just to see if these seemed to be placed in the system by docs or confabulators. As a physician, you can usually tell if the medicalese is real. And most of them are signed with names and addresses. They are very likely all genuine. That is all the time I had to go over those 37 – but please realize this system is also likely very under-reported.
And he is CORRECT – this is likely the most immoral thing I have ever seen in my entire career. I will promise you right now – this is going to be a disaster of epic proportions. Biden was very proud yesterday with his statement that “We are the only country giving these shots to under 5 year old kids” The irony in that statement is enormous. My feeling is that is not going to age well – and will likely be a nice campaign ad for the GOP in about 5 months. Mark my words.
America continues to be exceptional. And with Covid, in not very good ways.
.....
comments related to the above:
I believe the Publix issue has to do with their pharmacy staff not being trained to give small children injections rather than a principled stand on injecting young children with the covid vaccine. I imagine that’s probably the case at many large chain pharmacies.
Starry Gordon Sometimes one thing stands for another. That is, someone may not want to take an overtly principled stand because of the (sometimes) very high social cost of having principles. So one says, “I’m sorry, I just don’t know how to do this.” One must pick one’s battles.
IM Doc Interestingly, the Publix corporation is refusing to comment on this issue. If it were as simple as that, you would think it would be easy to just say so.
My cousin the pharmacist did allude to that – see his point b above. It is an entirely different thing to give inoculations to little kids. They squirm a lot and the anatomy is different. So I understand there may be some reluctance to get involved here. But I also got the the distinct impression from my cousin that there was just a lot of concern about safety issues going forward.
I think I should explain what I mean by “moral injury” and what is going through the minds of these nurses and pharamcists.
Some months ago, when the inoculations were opened up to the over 6 crowd, we had a vaccine injury incident with a young child that ended up on the front page of the paper. It was severe, and it has ended up being life changing for this young man. It is hard for big city dwellers to understand, but in a small town, we all know one another, we see each other all the time, we are part of each other’s lives.
The nurse that gave that kid his shot happens to be my patient as well. Words cannot describe the agony this person has been through. They believe they were the one who destroyed this kids’ life. They gave them the shot. There has been absolutely zero indication that anyone but the nurse thinks this, including the family and the patient, but they will likely have months and years of recovery. It is still awful to see them struggling with this. It will likely change their life too.
Picture the other employees in that office. Now we are giving this to babies. What if this happens to one of the babies I am giving a shot to? Am I going to be able to live with myself…..They say it is rare and these are perfectly safe – but look what just happened to so and so.
This is moral injury. This is as intense as it gets, but there are so many other examples that have occurred with multiple facets of this pandemic. America does not realize the precarity of their health care work force right now.
Back when I was a young doctor, when medical ethics and principles still had some sway unlike now, the professors who taught me about medical statistics and research were very keen on harming even one individual with a drug. Our first rule after all is First Do No Harm. And I remember all those years ago, in a medical statistics class of all places being asked to read this short story.
https://en.wikipedia.org/wiki/The_Ones_Who_Walk_Away_from_Omelas
It is ever more important today. The moral question being hammered into our heads by our professors back then is even more important today.
Just how many people is it worth to save for one child to be killed or maimed? How many make it worth it?
I have been haunted by this question and by my professors and classmates struggling with this question for weeks now.
How does the “slide” support IM Doc’s concerns about vaccinating children under 5? Assuming he is correct that there have been 175 US deaths of children under 18 since the start of the pandemic, the VAERS raw data suggests that there have been 275 deaths post-vaccination of people under 18 — but with no causal connection established between the vaccine and those deaths, just a temporal correlation. As IM Doc might put it, we know those 275 deaths occurred “following” the vaccine but we do not know if they were “because” of the vaccine.
Then the slide totals up the VAERS hospital/ER visits of people under 18 within 3 days of the vaccination (5,806), but there is no similar US hospital/ER visits total for COVID infected people under 18 since the pandemic started.
Perhaps IM Doc’s insight into VAERS data is beyond my ken, but I thought VAERS data is notoriously raw and requires a deep dive and many follow-up controlled studies to develop a high degree of confidence in what it means. I also recognize that some VAERS results are so extraordinary to militate stopping things right away. What have those circumstances looked like in the past and how do they compare to this situation?
I agree that the entire analysis is fraught where the under 18 vaccine recipient cannot knowingly consent to the inoculation, the profit motive can deeply distort Big Pharma’s testing protocol and study conclusions, and “politics” can put its thumb on the government scale of what vaccines are useful and to whom should they be administered.
But, again, are IM Doc’s data conclusions and the resignations of the three nurses justified here — based on the data cited? Where is the discussion of the data the vaccine manufacturer supplied?
Maybe the nurses are heroes and IM Doc a truthsayer, but is the data contained in the slide he relies on as compelling as he suggests, and where is the vaccine manufacturer’s data?
Yves Smith The entire premise of this comment is incorrect. VAERS is “Vaccine Adverse Event Reporting System”. Its purpose is to record bad outcomes from vaccines. These reports are initiated both by doctors and patients, that’s why IM Doc looked to see if he could determine what proportion were patient-submitted.
IM Doc has discussed privately multiple cases of vaccine injuries that he submitted to VAERS that were rejected, including one for a particular type of shingles (a known bad outcome) that the non-medially trained person processing the submission rejected because it wasn’t recognized as an effect (as in IM Doc using a more specific designation got it rejected). Similarly, IM Doc himself suffered a serious vaccine injury that required treatment at a tertiary medical center and took a long time to resolve. The specialist there immediately agreed it was vaccine-induced, said he’d already seen 400 cases like that, and VAERS refused to take them.
IM Doc First of all, the nurses did not resign based on this dataset. They resigned because they, like many of us, are suffering from moral injury and this was the last straw. I have left an extensive comment elsewhere here today to further elucidate what I mean by that. Maybe you could put yourself in their shoes. I really wish we would all do that more often than we have been.
The VAERS system is notoriously inaccurate. It is so underwhelming in its ability to perform the function asked of it that it has become a national tragedy. As I have repeatedly stated, the VAERS system is a good way to pick up signals. I have used it for years when the flu shot season begins and through those months to monitor if there is a sudden increase in reports. It is very helpful in this way. Unfortunately, because of massive under-reporting, it is completely unreliable as way to find out exactly what level of VAE we are having. I tend to view what is on VAERS as the basement with the ceiling unknown. As I stated yesterday, it is clear to me that the Moderna death and permanant disablity reports were almost assuredly all valid. They were not written by confabulators. I have spoken with the VAERS employees a few times during this and I get the strong impression that the ridiculous fake ones that are clearly a hoax are removed as soon as that is recognized. Many of these are clearly related to medical problems that are widely known now to be directly related to these vaccines. Young kids do not routinely get DVTs and other things that are reported there. At some point we are going to have to come to terms with the fact that these vaccines are indeed causing some of these issues. I have also reported here in the past and I will report again that the current system is not even close to the manner in which severe issues were dealt with in the past. In previous times, if I as a physician, called in a death or serious complication report to a federal agency, it was taken care of with the utmost of care. That has not happened a single time I have called them during this whole affair. That is another reason I feel these numbers are probably on the low side. I have heard similar stories from peers.
The vaccine manufacturer’s data? You must be kidding. They have not been forthcoming with anything. You really must not be paying attention. We would ALL love to have the vaccine manufacturer’s data. It would help us answer so many questions. But it will be coming out in a drip drip drip format for the next decades. Nowhere near fast enough to help us answer so many vital questions…..Why are our politicians not demanding it to be released immediately? Why are they not by executive order demanding it be done?
This new paper came out this month.
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4125239It has among its authors Peter Doshi one of the editors of the BMJ, Robert Kaplan, the Chief Science Officer for AHRQ and Sander Greenland of UCLA – who writes the best textbook about medical epidemiology we have right now. What I am saying – these are not poseurs.
Because the federal agencies and the pharma companies are refusing to collate and release data, these researchers did the backyard approach through other means. It is a fascinating piece of work. What they found is that more patients were suffering excess severe adverse events with both Pfizer and Moderna vaccines than were being saved from hospital admissions. You heard that correctly – more people had severe side effects than people being kept out of the hospital. The numbers were particularly tragic for Pfizer. The authors absolutely admitted that this was the best they could do with the available numbers. BECAUSE THE GOVERNMENT AGENCIES and BIG PHARMA HAVE REFUSED TO RELEASE DATASETS. THIS IS ABSOLUTELY TRAGIC IN ITS UNETHICAL BEHAVIOR. They ended the study with a plea to release the data and given their findings, the urgent need to break out the risk/benefit ratios for different demographics. ie do old people have a satisfactory risk profile while young people do not, etc etc etc. I will reiterate – none of these authors are slouches. They are in the top tier of folks in their fields. This has to be taken seriously.
We all know these vaccines do nothing to prevent transmission or infection. That is by now I hope evident to all. Therefore, the “killing grandma” excuse no longer has merit. If anything, the vaccinated seem more cocky and inclined for risky behavior. No, the only thing right now on the table is the individual risk mitigation for each individual child. And the numbers just do not add up for the BENEFIT of these which studies tell us is basically zero to take on the risk. This is especially so in this 0-5 age group. This is a critical time for the development of the thymus and T-cell immunity and we just do not know what these novel agents are going to do for sure.
It gets back to the question I placed in another comment today – that has been haunting me. How many people need to be saved for one child to bear death or disablement? It is a profoundly important question and one I have been wrestling with for weeks. We are not going to find that answer in medical statistics or databases. We are going to find that in our own hearts. And we better quickly start the process of examining our own hearts – this may rapidly become the issue of our time.
And yes Yves has revealed my own struggle this past year. I have been not inclined to discuss it because I did not want that to really influence anyone’s personal decision. I do believe the time has come to be forthcoming. My medical issues with the vaccine are on a continuum. It affects most people very mildly but some have a severe problem. I ended up with the more severe issue, but not the worst. This has been going on for more than a year. I did end up with one of my old students as my physician specialist at a major center. And he did tell me he has seen many people with this problem all over that continuum. The vast majority of them were mild unlike mine. Under his care, I am doing better but this has not been without issues this year. Just in the past month, I have begun to feel normal again. Fortunately, unlike so many others who have had a vaccine problem, I have not been gaslit. But my physician did share with me the same frustration I have with VAERS and our agencies. They just do not seem to be too interested in problems.
It is very clear to me that the dam is breaking in regards to the promises and the perils of these vaccines. I watched the questioning of Dr. Birx in the US House yesterday long enough to realize that the evasion and deception and misdirecting are soon to be over. I heard with horror as she described why they so missed the fact that these vaccines were not sterilizing because they had “hope” in them. We are all about to find out that hope should never be the sole determinant in any of these things. We “hoped” they worked – so we went about coercing vast swaths, ruining people’s lives and jobs, because we “hoped” they worked. This is absolutely not the medicine I know and love. I am so sorry that my profession is behaving like this. I would have never dreamed it possible.
Pediatrician4U Hi! Pediatrician of 25 years here. I’m sympathetic to the political leaning of this site, and had to jump in and say that the idea that there is mass hesitation or that “the worm in turning” in the medical community against protecting our children from covid with these vacccines is not correct. I’m willing to say “anything is possible” wrt the specific experiences shared here by the author of this post, but the idea that there is a movement among *medical professionals* (especially ID docs!!) against toddler vaccination against Covid is frankly laughable and makes me give a bit of side eye to the rest of this post. I had to share this reality check.
I work in a suburban purple area and of course among families, there is some vaccine hesitancy, but the medical professionals including all of the injection nurses are are strongly in favor of these vaccines and their potential to save lives. No one is resigning- we are *thrilled*. Covid has been the #4 or #5 cause of death this last winter among the ages 1-5 yr. It has killed more/mo than RSV or Influenza ever does. Your pediatric nurses and doctors are very happy that we finally have the chance to reduce this impact.
My professional recommendation is for god sake’s, please protect your child from Covid. Advocate for better public policy wrt ventilation and masking, etc, but PLEASE also take this simple and safe step.
Yves Smith I don’t mean to come down hard on you, but just because a situation is bad (having toddlers get Covid) does not mean a particular proposed remedy is good. But your comment comes off as if your need to be able to Do Something has blunted your critical thinking.
First, IM Doc spent 15 years on an Institutional Review Board, five years as its chair, and so he is intimately familiar with the drug approval process and the statistical reviews. He is adamant that these vaccines are being used when previous vaccines, like the one for swine flu, were pulled off the market at a far lower level of deaths and complications.
Second, it appears you completely ignored the information from the infectious disease specialist. With the 0-5 injection only having just started, meaning comparatively few toddlers have actually gotten the shots, they have killed more 0-5 year old children than Covid has over the entire history of the disease! How can you be in favor of them in the face of data like this?
Third, I expect IM Doc to address this himself, but I am highly confident his data set is bigger than yours. He was formerly a professor at a major teaching hospital, participates religiously in their various Zoom grand rounds and other information-sharing, as well as keeps up with his students, many of whom are at tertiary medical centers, and can give readings on what is happening there.
Fourth, if nothing else, you are ignoring Publix’s refusal to administer the vaccines to 0-5 year olds. They have over 1000 pharmacies. They can’t get enough of their staff to administer the shots to offer them.
Fifth, your geolocation belies your claim to live in a purple area. 4 of the services say you are in San Francisco. One says Boulder Creek, which is in the general area of Silicon Valley and blue. The last is Pittsburgh, where the city is a bit less blue but still rated as liberal, than Allegheny County.
IM Doc There have been interesting further developments in the story since the last writing. They thought they were going to have an enormous demand for baby vaxxes – but apparently the appts were only filled for one day and a few into the next. Now it is crickets. In other words, the parents seem to be deciding en masse to give this a rest for now. It seems very likely that the nurses will have their jobs back, because there will be no baby vaxxes in this county – or just sparingly, so that the supervisors can handle the babies if needed.
I am hearing similar reports all over the country – there is very little demand in the first week other than the very large cities.
This comment pretty much encompasses the talking points of the CDC. These issues the commenter brings up are similar in tone to how the CDC is describing the situation. Interestingly, there are entire states where there has just been a handful of kids in the hospital with COVID for the whole time. There are many towns like my own where we have never had a kid hospitalized through this whole time. Certainly not minimizing this – but I think we have to take a cold hard look at data as we were trained to do and really assess risk benefit ratios.
I am not going to write this all out – Vinay Prasad MD has 2 videos that I think spell it all out. I have but minor quibbles with what he says. Here is the thing – Do I agree with everything Dr. Prasad says? Oh no. But I am a student of science enough to know that he is doing these expositions from a good place – and he happens to be very congruent with my own reading of the literature. Unlike the CDC. The horror of horrors was earlier this year in the Supreme Court when a Justice used obvious bad data and misinformation to vote to maintain the vaccine mandate. This is an example of where bad science and repeating misinformed talking points can cause real harm.
Dr. Prasad discusses the obvious lies and distortions meant to scare parents into vaccinating kids – https://www.youtube.com/watch?v=ykwMAur0RTM And here in this video he goes through the evidence of benefits and risks to these kids from 0-5 for vaccination – https://www.youtube.com/watch?v=CJnOn6Phzfo. As a member of an IRB for 20 years – and a journal club attender for more than 30 – I can find nothing in these analyses that is invalid. If you are so intent on vaccinating the 0-5 – and so sure the benefits would outpace the risks – I would love to hear why.
I would ask your commenter another very important question – Why is it that countries all over Western Europe have had their medical regulating agencies say NO? – in a big way? Would this commenter engage with me – and go down the list of the FDA committee members that made this decision – and see how many of them may be corrupted with other arrangements with Big Pharma? – Is even one of them a truly independent adviser without conflicts of interest?
With regard to the worm turning and doctors not being concerned about this……a few things indicate that I am not just making shit up as implied here –
This is from Marty Makary MD – MPH – of Johns Hopkins Univ
This is his tweet in response to one of the above Dr. Prasad videos –
https://twitter.com/MartyMakary/status/1539616084139151360
There it is in black and white – he is guessing fully 40% of peds in rural areas will not be recommending this to their patients. That includes our pediatrician – who was vehemently telling us not to vaccinate our own kids – who are older than 5 months ago. And he was making very good sense when doing so.
And then this letter came out this weekend from a group of doctors including both Dr. Prasad and Dr. Makary – and as you can tell there are multiple signatories who are peds or ID docs urging a relook or reframing of the entire vaccination of babies scheme. I cannot say I agree with everything in that letter – but I certainly agree with the vaccination issue.
https://www.urgencyofnormal.com
I am not just making this “worm turning” up. There are literally thousands of American docs who have signed this letter. When I looked through just the first few dozen – there were multiple peds and ID docs. ID docs are indeed questioning this issue, regardless of what you say. I spoke with one personally on Friday.
You reference the ID doctor that made the comment in that conference. Please note – he is a dean of Infectious Disease in this country. As a young man, I saw him take up the armor when similar things were happening during the AIDS pandemic. He tolerated no bullshit from the CDC or Fauci or manipulating data. That is an understatement. He tolerated no bullshit from anyone when it came to patient care. What he did the other day – I would have expected nothing less. He is one of this country’s legends. But a key word is RETIRED. He has freedom. He does not need to be worried about being fired or punished. That is the problem. We cannot have a rational discussion about these issues other than the CDC talking points. Thank you for kindly reiterating them. It is now time for my generation to pick up the armor. As I discuss above – the uptake of the vaccines is apparently way lower than expected in many places in this country and that is because of the abysmal performance of our federal agencies. The trust in them in this country is cratered and will likely take years/generations to fix. This latest turn with the baby vaxx is no different. Unless we immediately began to demand complete transparency and a cessation of the propaganda, our entire profession and the health of this nation are at grave risk.
Pediatrician4U I didn’t realize posting an opinion to the comment thread that didn’t fall in line with the group majority would result in an attempt at doxxing. I didn’t think that’s what this site was about.
I think the author of the post will agree that your assertion in point #2 above is incorrect even if you take that slide at face value. According to that slide, how many children age 6mo-4yr have supposedly died of covid vaccine? The one we just started providing last week? The only children in that age range that have received the vaccine so far are the ones in the trials. Are you seriously suggesting that more children 6mo-4yr died during the trials (btw– NONE did), than have died of Covid disease itself?
I don’t usually use confrontational language like this, but I’m reacting to the tone of your response. I’m a pediatrician who considers themself quite anti-Big Pharma. I counsel honey over Robitussin. I dissuade families for falling for Pharma marketing of “toddler formula” (totally unnecessary btw– it’s just the drug companies creating and marketing a made up product you don’t need). But being against Big Pharma doesn’t mean I never prescribe a medication. Or recommend a safe life-saving vaccine.
Fwiw, i stand by my characterization of the town I work in (though it is literally the least relevant part of my comment- just some background).
flora You may be all you claim to be. Still, something seems off to me, something sort of ad-speak sounding about your comments. Maybe it’s just enthusiasm. But it does sound like a sales pitch. Probably just my quirky parsing of what I read. I’m not a medico.
Yves Smith First, it is false and an attack on this site to say you were doxxed. We did not publish your name, your phone number, your home or work address, or your e-mail. We found three different places from which you might have made your comment. Even if we take the one that is the best fit with your claim of purple (Pittsburgh), it has 4,900 doctors. The ratio of pediatricians to doctors nationally is about 6.5%. Applying that to 4,900 says there are over 300 pediatricians in Pittsburgh (and that is assuming you actually were in the city and not practicing somewhere else in the county). In other words, it is impossible to identify you personally based on what we said.
The comment about you being in a purple voting area was not “some background”. It was to try to undermine IM Doc’s using his experience in his very blue and very vaxxed county as not representative by presenting yourself as being in a less Democrat leaning area that was nevertheless toddler-vaccine-gung ho. So that was part of your argument, not ancillary information.
IM Doc in his reply to your earlier comment provides additional substantiating information that shows that many doctors and parents are skeptical of using this vaccine on toddlers.
And as for your effort to critique a slide from a former and highly esteemed Dean of Infectious Diseases, you appear to have a reading comprehension issue. The information came from the VAERS database. VAERS does not include clinical trial results, it is to report adverse results on vaccines in use. IM Doc said he even checked the 37 death and permanent disability reports about Moderna to see if they looked to be MD submitted or from patients. Their doctor-like use of medical terminology and writing style strongly suggested they were provided by doctors.
These deaths and other bad outcome are in the 0-17 age group in VAERS, which given that there are unlikely to be any adverse reports in the database from the shots that started last week, this effectively means it covers next older aged cohort, 5-17. You could look it up on VAERS yourself. They are almost certainly less fragile than toddlers. There’s no reason to expect better outcomes on average and good reason to worry about worse ones.
And the number of vaxxed 5 to 17 year olds is also likely to be lower than total toddlers exposed to Covid since it spread in a big way in the US (say early March 2020; by contrast, the Pfizer vaccine was not authorized for use on 12-15 year olds until late August 2021 and for 5 to 11 year olds, until the very end of October 2021. So we have less than a year with these vaccines for these populations, versus two years plus of Covid risk for toddlers. That means the time/population corrected level of bad outcomes is even worse than the simple comparison suggests.
I strongly suggest you reconsider your vaccine-for-babies enthusiasm.
IM Doc I think the ID doc’s point is that we have had less than 350 kids who have lost their lives to this virus and we have had the 250 deaths reported in VAERS at the same time in a much shorter time. No they were not 0-4 they were the older kids. He never suggested this was babies. Nor did I.
I tend to be on the very safe side with babies. So did the FDA in the past. See the story of Frances Kelsey MD to understand what I mean. How many pharma dollars did Dr. Kelsey have coming in on the side when she stood up for the kids of America? How many current members of the committee in the FDA that approved this are free of conflict? Should not the American people and certainly our kids have the assurance for this grave a matter that those in charge are free of conflicts?
As I stated, I looked through some of this deaths and they appear to be genuine. This is the next closest age range to whom we are dealing with here. There clearly are a lot more deaths than I am comfortable with. And have never seen any IRB be comfortable with that trade off.
And this safety is unresolved…..I will say once more that we had a severe safety issue in my community that all knew about. Never addressed in any way by the authorities and massive distrust was the result. And now they want us to vaxx babies with a minimal at best efficacy with that risk signal out there. Unfortunately, these are babies, and repeatedly saying the vaccines are 100% safe etc is just not going to cut it with the parents of America. The trust has been severely affected. I deal with this every day of my life like no other time in my career.
As I have stated before, it is leading to my own moral injury.
I would like for him and any others to listen to that Dr. Prasad video and point out their differences. That is where the debate should be had.
That is the issue at hand.
re: “…absolute risk of serious AE from mRNA vaccines exceeds the absolute risk reduction of serious covid-19 infection.”
I’ve run lots of clinical trials, and helped write some protocols: …. so, depending on the definition of “serious adverse event” {SAE}, I might prefer to have the SAE than to be so sick with covid that I wind up in hospital.
I think the headline would be likely to mislead the casual reader.
IM Doc I feel this is one of the most important studies put out in the past year. The more I have thought about it, it may be one of the most seminal papers in my career over decades.
They are fairly clear what their definition of sae is and not sure I would feel the same way as you do.
This paper is a direct result of the dissembling and obfuscation of Big Pharma and our government agencies. The authors used multiple back door approaches with multiple data sets to come up with these results because the real genuine data that would answer the questions remains under lock and key. It is an absolutely fascinating study on how one may get answers in more than one way. Indeed, this will be required reading for students on my IM rotation from now on. It is important in two ways. The fascinating ways they deduce this data and a warning for the future about trying to subvert science and hide data. We cannot allow this to go on.
And these are not just Twitter bot writers. They are quite frankly the shining lights of medical data studies and epidemiology. Sander Greenland writes THE medical epidemiology book used by medical students everywhere. His book sits proudly on my shelf. Doshi is the editor of BMJ, the last of the Big 4 with its reputation not in tatters, and Kaplan is the CSO of the AHQR. These people live and breathe math in medicine and how to do approrpriate trials. They are our supreme experts in this realm. This simply cannot be ignored. And as someone who has spent decades on IRBs and journal clubs, I am just blown away by this work.
And the basic end result is that they found many more had to endure side effects from the vaccines than the vaccines prevented hospital stays. Damning. And it was much worse for Pfizer. Furthermore, as they state, and is clear from careful reading, they very likely are very much understating the ratios and the effect is likely much larger. But they cannot know for sure. Because the raw data has not been released from either Pharma or our govt agencies. As far back as my original post more than a year ago on the vaxxes, I stated that was a HUGE problem with the initial studies. Something did not seem right and the only way to find out is the raw data. And here we are 18 months later and not a step further down the road. We now have lived experience that they are a huge disappointment in containing infection despite the “triumph” framing, and we have all kinds of red alert signals about side effects. And still no data. These vaccines have been coerced on our population. Our leaders must step up to the plate and demand the data to be released. There is no other way to get to the bottom of this. The authors of this study have laid out in the best possible way what we can know and they too are begging for the data to be released. They assert this is critical because the raw data can lead us safely to risk stratification for vaccine administration for demographics, something we cannot do even remotely now. We are blasting them into everyone.
Where is the data? How is withholding data consistent with science? Given all that is happening around us, why is this being allowed to happen? Why are we allowing these vaxxes in our kids without the most full picture of benefits and risks freely available to the parents and their doctors? Why is there not an Act of Congress or Executive Order to do so?
This paper, by these experts who cannot be ignored, is a blatant indictment of our current situation. And given the reputations of these authors, it is an indication of the shift happening in my profession about these therapies. We cannot allow our current status to continue on.
Joe Well If they are minimizing adverse events, why was there such a freakout about the very small risks of cardiac problems from the J&J and Astrazeneca vaccines?
square coats Indeed. The mrna vaccines have seemed stinkier and stinkier to me (not because of mrna technology per se but because of just about everything else).
Yves Smith How about the number of people at the FDA getting royalties from Pfizer products?
JBird4049 I am reminded of the company that made thalidomide, Grünenthal, which was founded by Nazi doctors who had prisoners for their often lethal tests during the war. The company not only quickly knew about the problem, they suppressed the information and kept encouraging thalidomide’s use worldwide because of the profits they were making. I have forgotten anything more about the mess except that the FDA prevented its use in the United States and IIRC the legal prosecutions in Germany ended in very lenient settlements.
Considering the past, it would be unsurprising to me if American officials were making bank off of the mRNA vaccines. I wonder what the people in the 1960s FDA would think about today’s medical establishment including its regulators.
IM Doc This is a story I tell every year to my students in medical history. Her name was Frances Kelsey, MD. She was the FDA official who through sheer will cut through all the hubris and crap and greatly minimized thalidomide in the USA. We all owe this women a debt of gratitude. Her name is largely forgotten today but not by my students. She is one of the greats and one to be emulated.
The NIH makes quite a bit of royalty from the Moderna vaccines. It is unclear to me how much Fauci and his top lieutenants are personally making – the news is a bit opaque – but I am certain if we have a GOP wave this year, that is all going to come out in the wash.
Not covid related, but since I've posted his comments related to his political sea change, here's another:
Actually no they are not rolling their eyes. I happen to be of the camp that this should be between a woman and their doctor. But I personally am pro life. This was one of the first indications that I was no longer welcome in the Dem Party. I was told to my face in front of others on multiple occasions that I was a horrible misogynistic mansplainer. Please note, I never one time have ever expressed a desire to get in the way of someone else who has different opinions to have an abortion. But because I expressed an opinion that I MYSELF would never be ok with a child I sired to agree to an abortion, I am worthy to be damned to hell. Now, I just never bring it up. I wonder how many like me out here who used to be reliable Dem voters are out here. I think it may be substantial. But it is hard to hear them through all the screaming.
You leftists can have it. The authoritianism in your actions is revolting to the vast majority of us in the middle. It is not just abortion. It is the entire framework of how you relate to the world. It is a form of authoritarian Manichaeism that is getting quite concerning. It is also fascinating to watch the many ways it is imploding on itself just as it has so many times throughout history. Your comment above, stripped of any nuance about this very complex issue, is a textbook example of Manichaeism. It does nothing but harden those of us who have struggled with this issue all our life that the Dem Party and its leftist core are not our home. The sad thing you cannot see through all the righteous screaming is that much of your base – the Latinos and the African Americans – have similar feelings that I do. I think November may be a surprise for you.
I am still struggling with the fact that my side of the spectrum has become far more authoritarian than the other side ever dreamed. It is unsettling. Even more so is the fact that the partisans on what I used to call my side cannot even seem to see the problem. The huge number of what I call New Deal Dems out here in the heartland who I have contact with regularly feel the same way I do. We need to start working on issues of the common working people and put the identity politics aside. They are absolutely toxic to a functional society.
“By abolishing longstanding legal protections, the U.S. Supreme Court’s reversal of Roe v. Wade serves American families poorly, putting their health, safety, finances, and futures at risk. In view of these predictable consequences, the editors of the New England Journal of Medicine strongly condemn the U.S. Supreme Court’s decision.”
Not every day the editors of the New England Journal of Medicine condemn a decision of the SCOTUS.
IM Doc I write this as a medical historian.
There may be very well thought out reasons why this ruling is bad. I am struggling with it myself. However, I know for sure that I will not depend on the NEJM for help with this issue. They do not have a very good record when you look at the big arc of history. They were avid supporters of things like eugenics, forced sterilization, and frontal lobotomies in the past among many others. These editorials are written not by actual practicing physicians but by the most ivory tower detached academics who would not know how to handle a patient in any way. The same is true today.
The NEJM should be used as a gauge of how elite physicians are feeling at the time it was written. And not of how something should be viewed going forward. Their opinions often appear quite embarrassing to the medical profession many years later. I often use these kind of editorials from decades ago for student readings. It shows us how the “cool kids” thought at the time and how ridiculous they sound now. It does not even have to be decades. Their editorial pronouncement that the COVID vaccines were a “triumph” 18 months ago seems a bit off today.
The column on Paxlovid being a failure on its own terms, with the terms of the trial hidden from public view, and approved in secret by the FDA, might get buried by all the justified Roe coverage, but this too is absolutely beyond scandalous. Social murder. (Peddling this drug to the exclusion of funding development for ones that might work, or do work today.)
An updated, more recent analysis from 1,153 patients (out of a possible 2,246 patients) showed a lackluster, non-significant 51 percent relative risk reduction. A sub-group analysis of 721 vaccinated adults with at least one risk factor for progression to severe Covid-19 showed a non-significant relative risk reduction in hospitalization or death (treatment arm: 3/361; placebo: 7/360).
…
But unlike Biogen, I couldn’t even find any online record of a meeting by Cavazzoni justifying the protocol amendment for Paxlovid, let alone an adequate one. Pfizer would have had to provide detailed reasoning in its protocol amendment and the FDA kept those requests and changes a secret. It’s just another example of the FDA’s total lack of transparency.
https://www.theamericanconservative.com/articles/biden-pays-big-bucks-for-pfizers-latest-flop/
It’s too bad the author is all-in on herd immunity, but the information on Paxlovid is nonetheless damning.
This country is in terminal decline.
IM Doc Over the past month, I have had some experience with Paxlovid. Enough to confidently make a few observations. We have been using it for patients who are higher risk because of age and medical issues, and only those who are not on contraindicated meds. So a fairly substantial number.
1) It really does not work all that well. Indeed, many patients do not feel better at all after several days. They often feel much worse. I have had multiple couples and families where one spouse demands Paxlovid and the other demands VitI/flovoxamine/some kind of steroid/NSAID – and invariably without exception – the second group does better much quicker. This is observational, case record level data – but is entirely consistent with what I have seen before in the pandemic. Again, the fact that all of these other agents have not been studied in any kind of trials but what are known as “show trials” IOW meant to fail – is an indictment against our medical agencies. This will not age well.
2) I have now had a handful of these “rebound” cases. Without exception, they are significantly more ill on the rebound – and this is 10 or so days later. There was an initial burst of discussion about this but again, now, as usual, crickets. I have no idea what this rebound phenomenon means. But it is a very real phenomenon.
3) It is very expensive. 700 dollars or so per course. It is being covered and paid for – but SOMEONE is paying for it. And again, the paltry effect does not seem to be worth the billions being spent.
4) Lots of dropouts. It makes many patients feel much worse in so many ways within just a day or two that they just stop taking it. I have some very serious qualms about this given the fact that this is absolutely what we are NOT supposed to do with antivirals. This kind of behavior is what leads HIV patients to become resistant to HAART. But there is a significant minority of patients who just feel so much worse they quit taking it.
5) There is absolutely no help with reinfection guidance from our agencies. I have so many patients now who are having 3 or even 4 reinfections that it is becoming hard to keep up with the numbers. Invariably, they are sicker each time. Majority are certainly not hospital level – but we are headed that direction if this keeps up. And so many of these people have already had a course of paxlovid on the last reinfection that may have just been 4 weeks ago. ( I view this as a completely different issue than the rebound – that very clearly happens within 6-10 days). No guidance on this at all – do we give them a second round of paxlovid this close after the first round? What is that going to do with viral resistance? What do you want me to tell these many patients who have had both vaccine and paxlovid failure – they are becoming very angry…..I am getting so used to being the whipping boy for the patient’s frustration. And I really cannot fault them – they have very valid points.
6) Getting back to patient anger and hypocrisy. I have just gotten to passively shaking my head when I see the usual tweet from one of our politicians – So and So, I have my 3rd bout of COVID – but thank God I have been vaccinated and boosted, you should be too. Things would be so much worse for me now, but because of my vaccination status, I have very mild symptoms. Nevertheless, the PAXLOVID I am on will help me too.
DO YOU NOT UNDERSTAND YOU ARE COMPLETELY HYPOCRITICAL in THIS STATEMENT – This drug is only to be given to those who are high risk. That does not include Justin Trudeau, Pete Buttigieg or Jen Psaki, Gavin Newsom or Kamala Harris among many others. All of whom have made variations of the above statement. (I do not include Dr. Fauci in this list because of his age he actually is high risk). First of all, if you are legitamately getting Paxlovid – your symptoms must be much worse than you are letting on. Secondly, this is very very poor modeling behavior. You as politicians should be modeling the CORRECT thing for the world. What you are doing is undermining the entire project.
There are days I want to just give up.
The anti-abortion movement, including electing anti-abortion candidates and appointing an anti-Roe judiciary, has been going on for 50 years. The participants in that movement are responsible for this decision. They don’t get to blame it on proponents of vaccine mandates, whatever else one may think about that issue.
IM Doc I am so sorry – but one of the most important aspects of medical ethics is that the principle in question must be universal in its usage and understanding. A principle of medical ethics simply cannot be applied to one issue and then not another. The resulting moral chaos will become destructive very quickly. This is just the way it is.
One side can simply not vehemently use medical ethics principles on its pet issues and then ignore the same on those they oppose.. That would make them moral morons as is being evidenced today. The hypocrisy from the very same politicians is just overwhelming. They look life fools.
I do not think anyone is blaming the loss of Roe vs Wade on the proponents of vaccine mandates. I think they are rightly pointing out that the hypocrisy on display is revealing to all involved that ignoring ethical principles in critical medical issues in our society that they have screamed from the rooftops for years really makes them look like zeroes. I will assume from this day forward that someone like Elizabeth Warren is a moral zero until proven otherwise. She clearly is unable to rationally parse through an ethical dilemma. It pains me to say that. But she has been proving this with so many other issues over the past two years that this seems like nothing. The same can be said for many others I used to respect.
Since both abortion and vaccine mandates of a non-proven, no-safety record substance are both medical issues – both must be evaluated on medical ethics in exactly the same way. You simply do not get to be ethical on one issue and not the other. Unless, of course, your name is Joseph Mengele or many others throughout history who have – and we all know the consequences.
This is absolutely fundamental to medical ethics.
The issue of “my body, my choice” goes right to the heart of medical autonomy – one of the most important medical ethics principles there are. It is absolutely relevant to abortion – but equally relevant to the mandate issue as well. Again – the fact that this has rightly been used for generations now for the abortion issue – and then tossed out the window in a heart beat for the other side speaks volumes in the hypocrisy for the side doing it.
The big bugaboo with medical autonomy in the hundreds of debates I have been witness to over my life – is what about the autonomy of the fetus?…..When does a fetus have autonomy?
The other issue that gets less press but is equally important – is “this decision is between a woman and her doctor”. That issue goes right to the heart of medical privacy – another ethical issue that was tossed right out the window by the mandate crowd – the same ones who have been chanting it for decades. I would love for you to come and talk to a patient of mine – a young woman with a clotting disorder – who came to me to discuss her options with the vaccine mandate at her work. Together ( a woman and her doctor) came up with the decision that these were not a good idea for her. I filled out a medical exemption. It was summarily dismissed by the employer. She got the shot – and 2 days later had a massive PE. Thankfully did not die. But the same people who are now screaming about this issue with abortion were all over her facebook feed demonizing her for even thinking about getting a medical exemption – she showed it to me – tears in eyes – “these people are my friends.”
Sorry – there is no other way. Medical ethics are non-negotiable. They are not for some issues and not others. Failure to understand this is why we are in the mess we are today. The few medical ethicists that came out to support these mandates were simply unable to make their case. And as is always the case with the truth – it will eventually come to light.
I struggle with the abortion issue mightily. I read posts like the one above – and I get it. I have had decades as an instructor in medical ethics to go over this in my mind and soul. But what has happened in the past year has demonstrated to many people that the moral and ethical fiber in this country is very thin indeed.
About the foreign trip.
I had the Biden remarks to NATO on TV this AM – and it was all about NATO and Russia.
And then something happened that just rocked me. As in I will never trust Biden again – nor basically his party until the clean sweep is done. During the NATO Russia speech in front of the leaders of the free world, Biden took a fairly deep swipe at the US Supreme Court and them being against human rights and specifically mentioned Roe v Wade.
What the hell does Roe v Wade have to do with NATO or Russia? Does anyone else seem to see the supreme irony in comments like that spoken to the European nations – who almost to the one have MORE RESTRICTIVE abortion laws than many of our US States.
Call me old-fashioned. But I do remember a time when it was absolutely looked down upon for any American politician to go onto foreign soil and talk down to the world any other politician or any other political instituion. And yet – he goes onto foreign soil and makes this kind of comment about the US Supreme Court, and equal branch of government – at least the last time I checked.
Totally classless and totally disrespectful of centuries of precedent.
I, an officially former Dem, am rapidly becoming a member of the “I will crawl over hot coals” to vote these people out. They are not worthy of the position. Furthermore, my wife especially, has begun to make donations to the other side – she is so horrified. It is also official – after more than 5 decades between us being Dems, we are no longer. Our official party registration was changed on the first day it was able to be done in our county today. And my God, the place was packed with people doing the same thing.
I am so very disappointed with my party. I cannot believe what they have become.


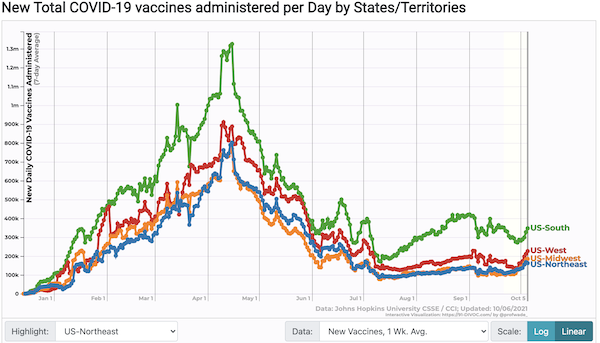
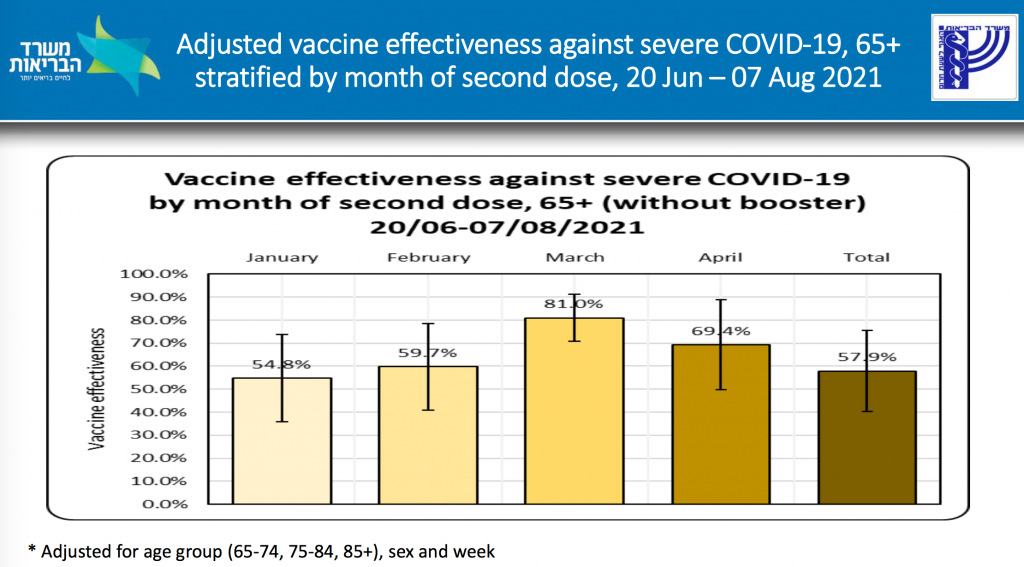
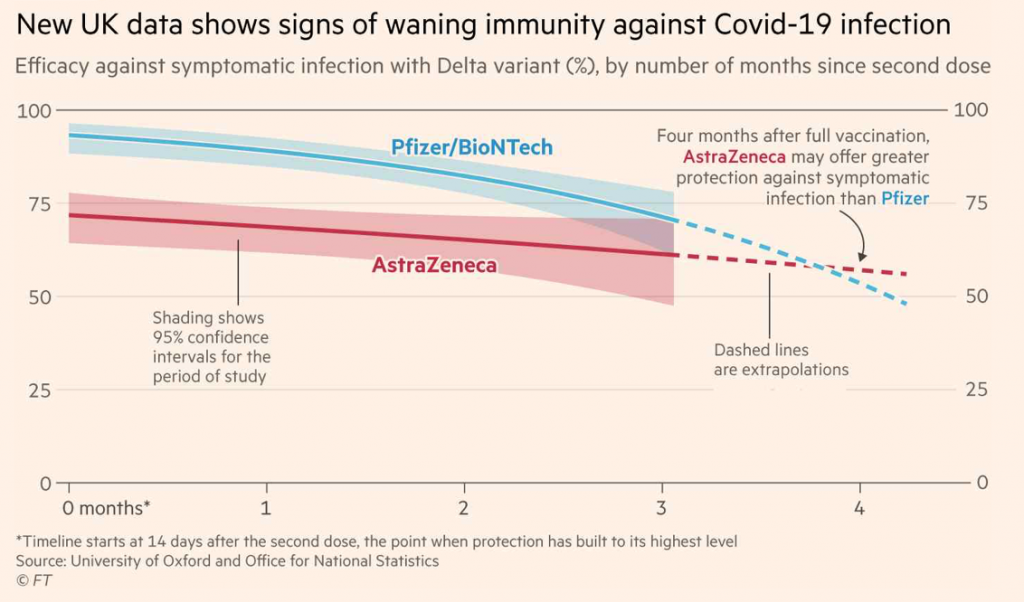
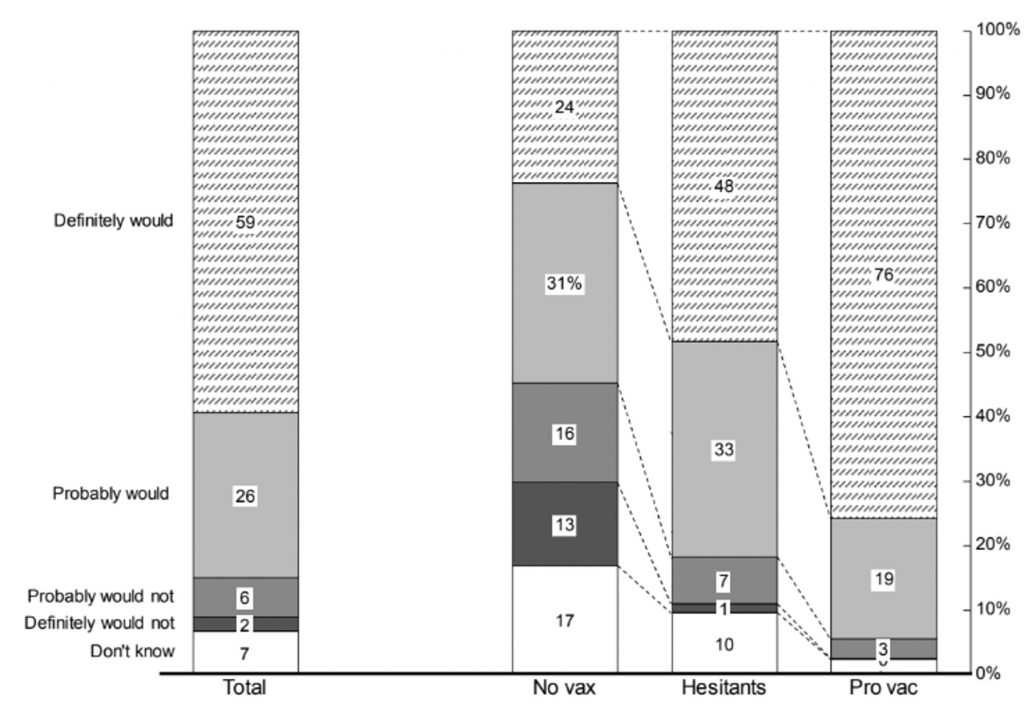
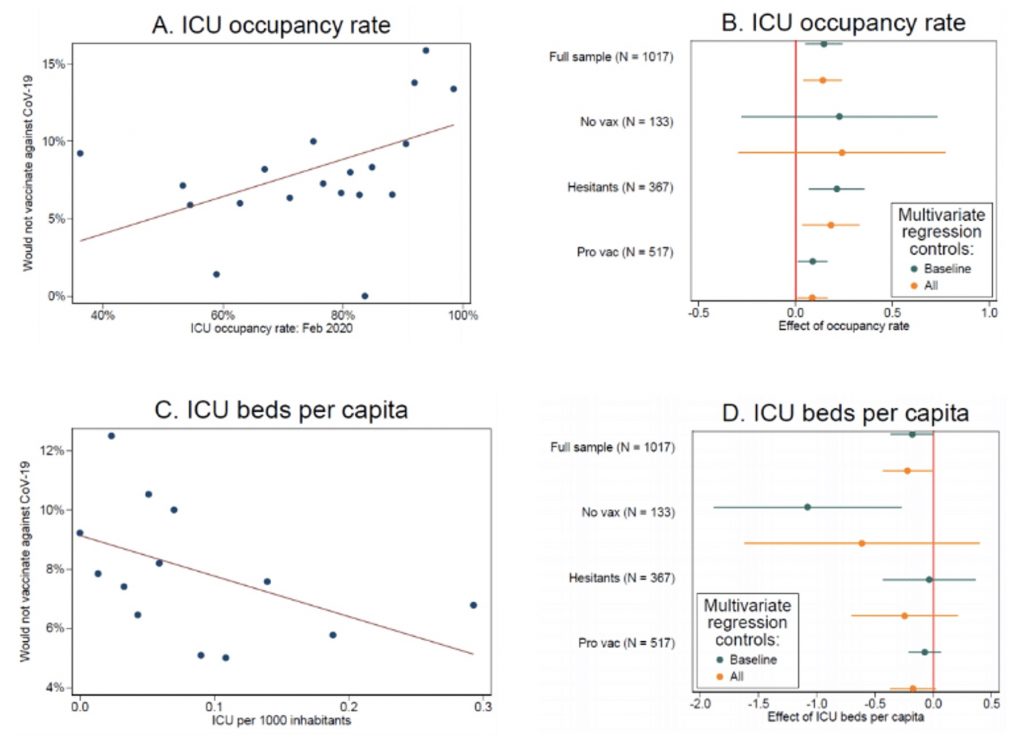
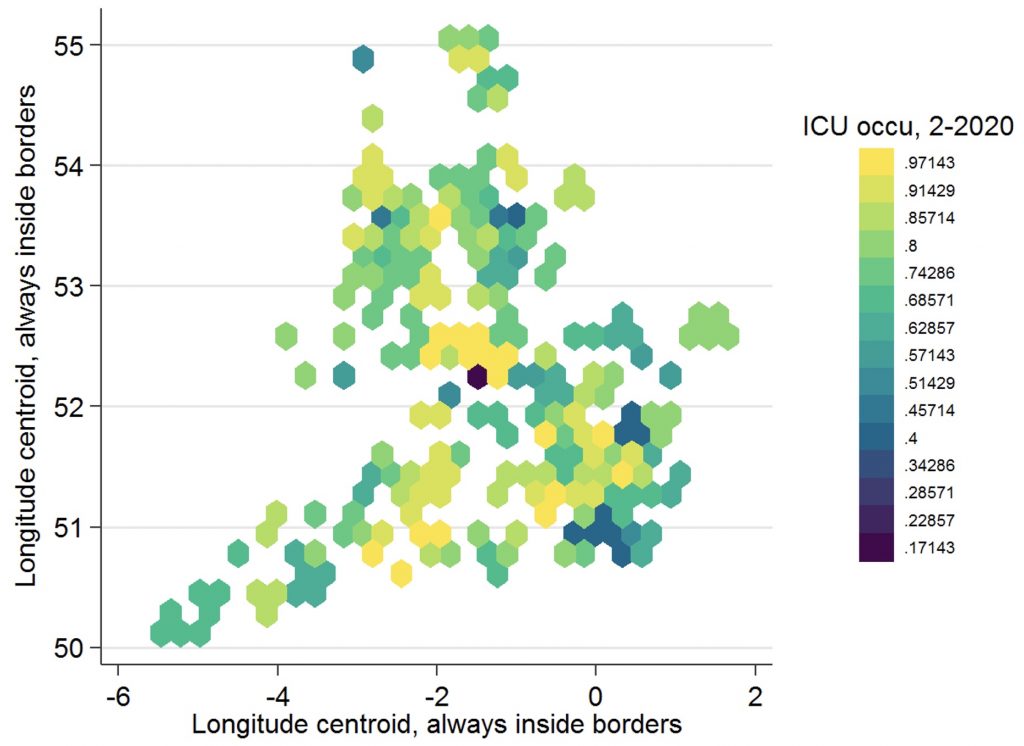
I’m curious if these children’s parents have to sign an EUA absolving the vax makers of any liability?
No
I’m pretty sure you ae wrong.
https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-moderna-and-pfizer-biontech-covid-19-vaccines-children
8 days ago — For the Pfizer-BioNTech COVID-19 Vaccine, the FDA amended the EUA to include use of the vaccine in individuals 6 months through 4 years of age.
You are incorrect, the only version of the Pfizer and Moderna drugs sold in the US is the EUA version.
Just try calling your pharmacy and asking if/when they will have Comirnaty, the FDA approved version of Pfizer. I guarantee they still have no date.
EUA drug = waiver has to be signed.
Well I didn’t at my pediatricians office for whatever reason
He was remiss. I am pretty confident any hospital or pharmacy chain administering the vaccine would.
If this is the case, your pediatrician is seriously setting himself up for liability. Despite the fact these were approved in August, they are still using the EUA version. There is no explanation on offer. This is very alarming behavior.