IM Doc pt11
Aug. 31st, 2021 05:42 pmIt’s Time To Talk About Ivermectin
I’d like to start this article with a couple of disclaimers and a caveat. First of all, I am not a medical doctor. This article is not intended as medical advice. It’s a layman’s account of how an extremely cheap, safe and widely available off-patent medicine called ivermectin appears to be saving the lives of countless Covid-19 patients across Latin America and beyond. Yet hardly anybody is talking about it.
Here’s the caveat: The first section of the article, which was completed on Friday, is about Mexico City’s recent deployment of ivermectin in its fight against Covid-19. On Saturday, Mexico’s Ministry of Health jacked up its total excess death count due to Covid (for the whole country) by 60%, from 182,000 to 294,000. However, most of these deaths took place before Mexico City began using ivermectin as part of its its test-and-treat approach to Covid.
Covid-19 vaccines are reaching most emerging and developing economies in only drips and drabs, with a few notable exceptions such as Chile. In many countries, locking down entire cities or regions and paying millions of non-essential workers not to work while front-line doctors and nurses battle to contain the virus is not an option. There simply isn’t enough money available. This has left doctors and health authorities with little choice but to try out cheap, widely available generic medicines. Those drugs include ivermectin, a “well-studied, well tolerated,” (in the words of a 2013 FT article) off-patent anti-parasitical.
The results have been extremely promising, according to almost all of the clinical studies conducted thus far. Many of the studies took place in Latin America where around half of the countries in the region have used or are using ivermectin to some degree or another. A meta analysis of 42 clinical trials, involving approximately 15,000 patients, found that 83% showed improvements with early treatment, 51% improved during late-stage
treatment and there was an 89% prevention of onset rate noted. Yet the studies have received scant attention in more advanced economies — so much so that the vast majority of the people I talk to here in Europe have still not even heard of the medicine.
Bucking the Trend
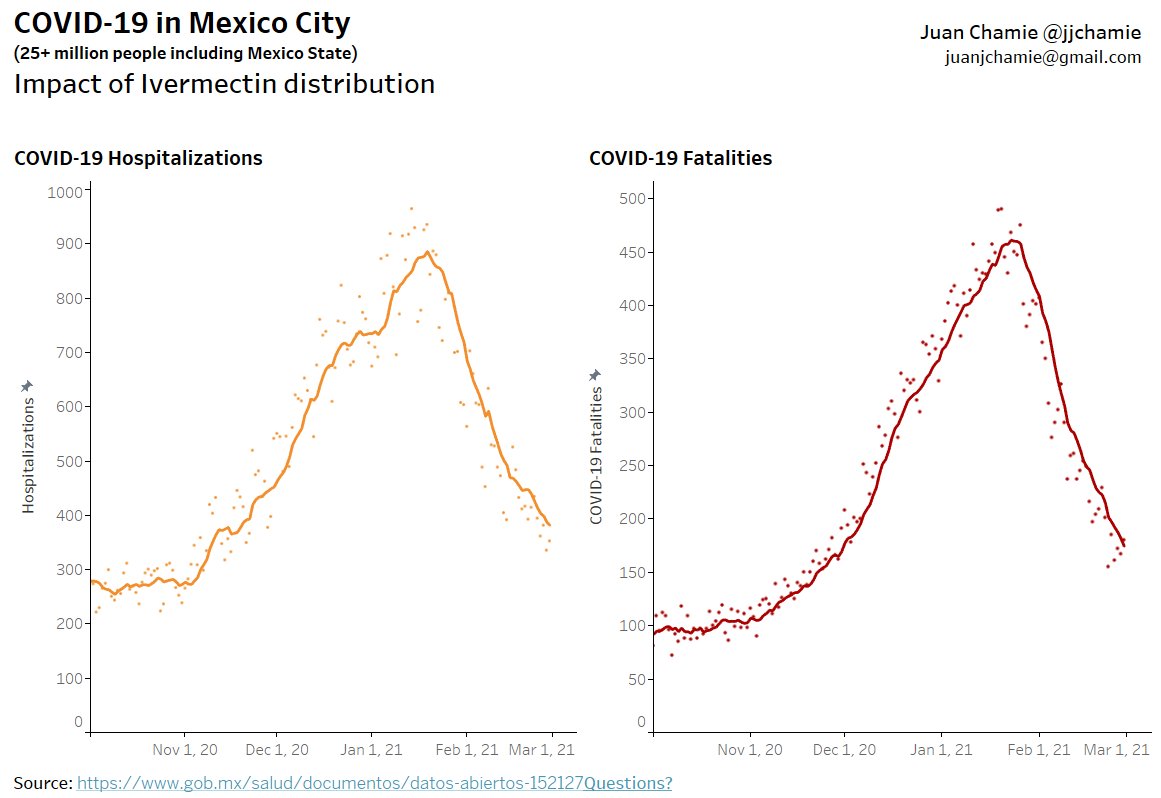
On December 29th of last year, Mexico’s Institute of Socal Security (IMSS) allowed ivermectin to be prescribed to outpatients with Covid. On the same day the Secretariat of Health of Mexico City and the State of Mexico decided to adopt a protocol in which anyone testing positive at any one of the city’s 250 rapid testing sites would be given ivermectin. As you can see in the graphs below, courtesy of Juan Chamie, a data scientist from EAFIT University in Colombia, based on data provided by Mexico City authorities, the number of hospitalizations due to Covid and excess deaths peaked shortly after the New Year and have been falling sharply ever since. They are now almost back to their prior base line.
Mexico City is the first major global city to adopt what amounts to a test-and-treat approach to covid-19 involving ivermectin. But it was the largely indigenous southern state of Chiapas that led the way last summer. In July 2020, as Mexico was buckling under its first wave of the pandemic, the state decided to distribute ivermectin as a Covid-19 treatment, having already deployed the medicine in its battle against mosquito-borne RNA viruses such as Zika and Chikungunya. Since October Chiapas has consistently occupied the lowest risk level on the federal government’s coronavirus stoplight map.
Thanks to ivermectin’s apparent success in Chiapas, IMSS allowed the medicine to be prescribed nationwide. It also helped launch the pilot program in Mexico City, for which it received a barrage of criticism. An official group of health experts argued that there’s no scientific evidence that the drug is effective, and called for the immediate repeal of its use. To their credit, both the Secretariat and IMSS have stuck to their guns.
Playing With Lives
Of course, there’s no way of definitively proving that the rapid falloff in hospitalizations and deaths, first in Chiapas and then Mexico City, is due to the use of ivermectin. Correlation, as we well know, is not causation. It’s also true that Mexico City authorities have introduced tougher social distancing measures and travel restrictions since December. But similar dramatic drop offs have been witnessed in other regions and countries where ivermectin has been used widely, including across the length and breadth of Peru and Iran as well as parts of Brazil, Paraguay, Bolivia, the Dominican Republic and India.
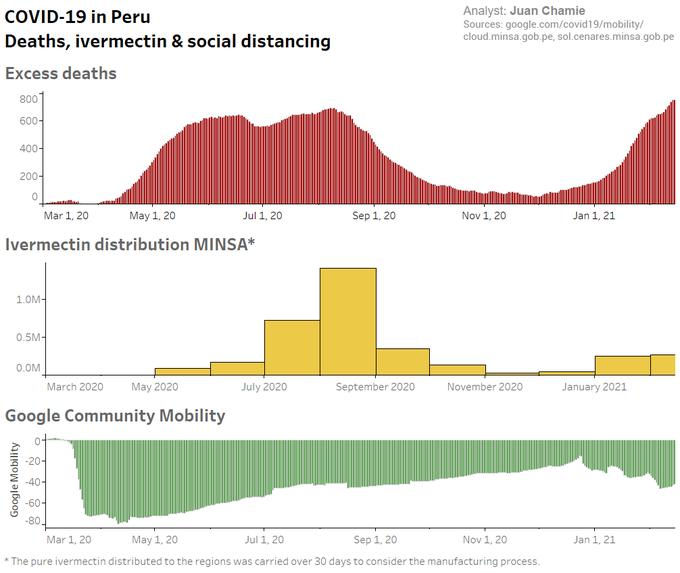
In Peru, ivermectin was used in eight states during the very early stages of the pandemic (May-July). Its use was then extended to the whole country except Lima, which did not start deploying the drug until months later. For the 24 states with early IVM treatment (and Lima), excess deaths dropped 59% (25%) at +30 days and 75% (25%) at +45 days after day of peak deaths. But in October, after the first wave had been brought under control, the new government in Peru took the inexplicable step of withdrawing a number of medicines, including ivermectin, from its treatment guide for the disease. Within weeks hospitalizations and deaths were soaring once again.
The following graph, taken from a study by Juan Chamie, Jennifer Hibberd of the University of Toronto and David Scheim of the US Public Health Service, shows the sharp rise, fall and resurgence in excess deaths (among the over 60 year-old cohort) in Peru as the virus waxed, waned and waxed again. Between August and December case fatalities dropped sharply in all states but Lima, yet six indices of Google-tracked community mobility rose over the same period, before rising once again. In other words, the treatment appeared to be working even as the country reopened.
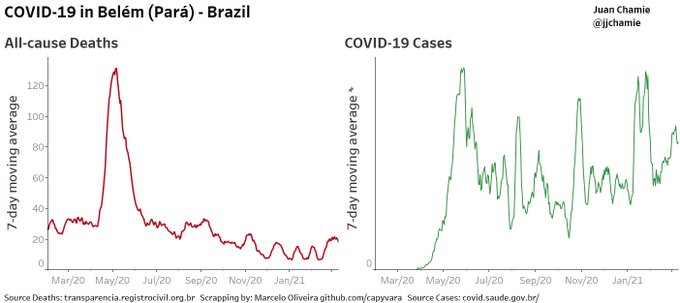
In the Brazilian city of Belem authorities began using ivermectin way back in June 2020. Since then the city has managed to escape the massive surge in covid-related deaths that has plagued Brazil since early November, as the graphic below shows. In another study a like-for-like comparison of cities in similar regions of Brazil showed that the cities that began distributing ivermectin in June last year were, by September, registering much lower case counts than those that didn’t.
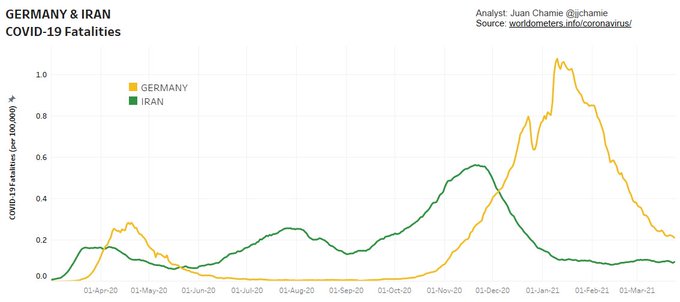
Iran has also seen a sharp fall in covid-related deaths since late November followed by a flattening of the curve. Earlier that month the country, with a similar population to Germany and an urban population density twice as high, succeeded in gaining the technical knowledge to produce ivermectin and began distributing it to hospitals in the country.
What is Ivermectin?
First discovered in 1975 and launched onto the market in 1981, ivermectin is a safe, broad-spectrum anthelminthic drug registered for the treatment of a number of neglected tropical diseases (NTDs) including river blindness (onchocerciasis), strongyloidiasis, trichuriasis, ascariasis, and lymphatic filariasis. It is also used widely in veterinary medicine. In recent years it has been discovered to have strong anti-viral properties against RNA viruses such as zika and yellow fever. In its use against river blindness in Africa it is estimated to have prevented 7 million years of disability.
The medicine is not only extremely effective in treating a broad range of illnesses, including RNA viruses; it is also well tolerated. To date, more than 3.7 billion doses have been distributed with an excellent safety profile. Most adverse reactions are mild, transitory and associated with parasite death rather than with the drug itself.
“The reason why this medicine is distributed in Africa not by doctors and nurses but mainly by volunteers is that it is extremely safe,” says Japanese microbiologist Satoshi Omura, who jointly with the Irish parasitologist William C. Campbell, led the team that isolated a strain of Streptomyces avermitilis that produce the anti-parasitical compound avermectin, the active ingredient in ivermectin. Omura and Campbell were awarded the Nobel Prize for Medicine in 2015 for their discovery.
Dr. Omura himself believes there’s already enough evidence of the benefits of ivermectin against Covid-19 for it to be granted approval as a therapeutic. One of its biggest benefits is that it appears to work in the early stages of the disease, he co-writes in an article published earlier this month in the Japanese Journal of Antibiotics:
“Currently, there are no therapeutic agents available for mildly ill patients who are being treated at home (or in self-isolating accommodations) or for moderately ill hospitalized patients. Nothing is as helpless as a disease without a cure.”
Anti-Viral, Anti-Inflammatory, Anti-Long Haul
Another major ivermectin proponent is the Frontline Covid-19 Critical Care Alliance (FLCCC), which has been trying to repurpose medicines already on the market for the treatment of Covid-19. In October it created the I-MASK+ protocol for prevention and early outpatient treatment, which includes ivermectin, vitamin D3, vitamin C, zinc, melatonin and quercetin.
The FLCCC believes that ivermectin is not only “one of the world’s safest, cheapest and most widely available drugs,” it is also the most effective against Covid. “The studies we presented to the NIH revealed high levels of statistical significance showing large magnitude benefit in transmission rates, need for hospitalization and death,” says Dr. Pierre Kory of the FLCCC, who twice gave testimony to the US Congress on Covid-19.
Besides the dozens of clinical studies conducted so far on the efficacy of ivermectin against Covid, the FLCCC also cites “natural experiments” in Peru, Brazil, Paraguay, the Dominican Republic and Mexico where ivermectin was distributed widely, with “large decreases in case counts … soon after distribution began.”
Another recent convert to the cause is Dr Alessandro Santin, a renowned cancer researcher who runs a large laboratory at Yale. Santin believes that ivermectin is a game-changer that could significantly reduce Covid’s toll on human health.
“The bottom line is that ivermectin works. I’ve seen that in my patients as well as treating my own family in Italy,” Santin said, in reference to his father, 88, who recently suffered a serious bout of COVID. “We must find a way to administer it on a large scale.”
In an interview with Italian daily Il Fatto Quotidiano, Santin explains why he believes ivermectin is so effective against Covid:
- Its powerful anti-viral properties: “The theory behind the main mechanism of action is that ivermectin attaches itself to Sars-Cov2’s Spike1 protein as well as at various strategic points used by the virus to bind and enter our cells. This is why it can also work against variants, unlike monoclonal antibodies.”
- Its anti-inflammatory activity: “Ivermectin has a powerful anti-inflammatory effect similar to that of cortisone. But unlike with cortisone, the effect is not immunosuppressive. Therefore the immune response of both T cells and B cells (producing antibodies) continues to function under ivermectin, acting on the transcription factor NF-KB (which informs our body to produce cytokines and causes a real cytokine storm when hyperactivated by Covid). This is why the drug also works well during the advanced phase of the disease”.
- It even seems to help long-haulers: “I have treated and am treating ‘long haulers’, including people who have been sick for a year and who do not breathe well, who have tried out everything to no avail. Within two weeks of starting them on ivermectin… these people have started to live again, with practically no side effects. The virus is an intracellular parasite; only if it enters our cells can it use the cellular machine to replicate. If it can’t get in and hack our immune system, then it stays out on the doormat and gets attacked by our immune system much more easily.”
More Evidence Needed, Say Regulators
Yet despite the growing body of evidence supporting ivermectin’s therapeutic effects against SARS-Cov2, national and supranational health authorities, particularly in more advanced economies, are dragging their feet. The European Medicines Agency (EMA) concluded this week that the available data “do not support its use for COVID-19 outside well-designed clinical trials”. The decision comes just two months after Slovakia and Czechia became the first EU countries to approve the temporary use of ivermectin against Sars COV-2.
In the US Ivermectin is not yet FDA-approved for the treatment of COVID-19, but in January the NIH changed their recommendation for the use of ivermectin in COVID-19 from “against” to “neutral”. This is a major step forward. As a result, doctors are at liberty to prescribe ivermectin for Covid patients.
But most regulators and expert panels insist that definitive proof is still lacking, despite the abundance of real world data, and have called for randomized placebo controlled double blinded studies. But that is time consuming and time is a luxury most doctors and their patients can ill afford right now. As covid continues to rage and patients continue to die, growing numbers of doctors feel that the risk of doing nothing, particularly in the early stages of the illness, significantly outweighs the risk of doing something — especially if that something has already been shown to work across multiple trials and real-world experiments.
“Clinical trials take time, but because of the abundance of overseas data, it may not be necessary to conduct clinical trials in Japan,” says Omura. “Experts have shown the numbers and announced that they are working. Therefore, I would like [the Japanese health authority] to grant it special approval. If you do not use it here, what is the special approval system for? Some people will die if they are waiting for a clinical trial.”
According to a WHO-sponsored review and meta-analysis of 18 clinical studies, the drug could cut the number of deaths from Covid-19 by as much as 75%. Crucially, some of the studies suggest that it is effective not only as a treatment in the early and later stages of the virus but also as a prophylactic. Yet the conclusion of the WHO-sponsored review is that more studies are needed.
Contrast this with the FDA and EMA’s mad rush to approve the anti-viral medicine Remdisivir for use against SARS-CoV-2 last October, despite the medicine’s lackluster performance in clinical studies and unproven safety record. On October 15, results from WHO’s Solidarity trial suggest that remdesivir does not even reduce mortality or the time COVID-19 patients take to recover. Yet a week later the FDA approved the drug for use against SARS-CoV-2 in the US, becoming the first drug to receive that status.
With a five-day course of treatment costing around $2,600 per person, there’s a lot of money to be made for remdesivir’s manufacturer, Gilead. Once remdesivir was approved in the US and the EU, it set off a cascade of approvals across the world, including in countries such as Brazil and Mexico whose public health systems cannot possibly afford to administer it on a large scale. In this case that is a good thing given how ineffective the drug appears to be.
Meanwhile, a Nobel-prize winning medicine that has been used extensively for four decades and costs just a few dollars per course of treatment could prove to be one of our best lines of defense again covid. Time and again it has been shown to work. Yet for the moment most health authorities in advanced economies — and quite a few in less advanced ones (South Africa, the Philippines, Peru…) — do not seem to be interested. In the coming days the World Health Organization is expected to come out with a definitive recommendation for or against ivermectin. If it opts for the latter, the pressure on doctors to stop using it will only increase.

John Day, M.D., “Treat Your Own COVID” — article in The Automatic Earth:
… Ivermectin has a remarkably broad safety profile, and has been served up about as many times as McDonald’s hamburgers, to man and beast alike, for various forms of worms and parasites. It does cause birth defects in rats, when given at high doses, so don’t use it in pregnancy, please. Like most medicines to treat coronavirus illness, ivermectin does different things against the virus, than it does on regular days. Ivermectin inhibits the transport of the viral RNA into the cell nucleus, where it would be transcribed, manufacturing new viruses. It does other things, like reduce inflammation during cytokine-storm, in the second and third weeks of illness, helping the people who get really badly sick. Ivermectin is effective in prophylaxis, in early illness and also in later, severe illness, and through multiple mechanisms. Ivermectin is what I prescribe since last August.
Ivermectin is now available mail-order from India, and from a reliable source. https://www.medicinesdropshipper.com/antiparasitic-drugs.html#iverlast-12mg-tablet
The preventive, “prophylactic” dose of ivermectin is based upon body weight, and it can be taken weekly, once an initial level inside of the cells is established. Ivermectin leaves the cells very slowly, so it can just be topped-off once per week. There are some slight variations on this, but I’ll describe the one I prescribe. It uses the same body-weight dosing that you will find wherever you look up ivermectin dosing for humans or animals. For every 5 kg, or 11 pounds of body weight, a person takes 1 mg of ivermectin at that dose. For most people I treat, that is 12 to 18 mg of ivermectin per dose. For COVID-19 prophylaxis, this dose is taken Day #1, Day #2 and then every seventh day after that. If you forget, take it when you remember, and get back to the original schedule after that….
https://www.theautomaticearth.com/2021/02/treat-your-own-covid/
I learned about ivermectin’s use for Covid from Chris Martenson at Peak Prosperity at least six months ago. Through him I also became aware of Dr. Pierre Kory and Paul Marik at Frontline Covid-19 Critical Caregiver’s (FLCCC). They were using ivermectin clinically and were having great success. Dr. Tess Lawrie at Evidence-Based Medical Consultancy in Bath, England became aware of ivermectin when she watched Dr. Kory’s testimony at a Senate sub-committee hearing. She and her staff took it upon themselves to do a meta-analysis of ivermectin and found that it was significantly effective for all stages of Covid and as a prophylaxis. At the same time, the World Health Organization hired Dr. Andrew Hill at the University of Liverpool to do a meta-analysis of ivermectin which is now completed. WHO is supposed to be issuing a statement concerning ivermectin shortly.
I visit Naked Capitalism everyday and would notice an occasional article about ivermectin in the Links or Water Cooler. But I was disappointed that no major article on ivermectin was forthcoming. Until today. Nick’s article is excellent. The cat is now out of the bag. Evidence from around the world is showing that ivermectin is safe and effective against Covid-19.
> Dr. Tess Lawrie
Lawrie article (not peer-reveiwed) and video interview. Here is Lawrie’s company.
I believe this post and the comments are perfectly emblematic of unfortunately where my profession is and where my country is. I have to admit, I would have never dreamed this possible just 10 years ago.
I will start by quoting one of my medical professors years ago when I was an intern….You have to imagine it in a very hard Danish accent….”Young man, if research or scientific findings make you angry in any way, you must immediately examine yourself. You are by definition not practicing science or medicine, you are practicing dogma. You must put down your test tubes and go to the nearest closet and in private examine your soul.”
I have thought of this old man often this past year – and the tenor of some of these comments have brought him yet again to mind.
We have created a world where every side has their own facts. Unfortunately, I believe we are all going to find the hard way that science is not going to work like that.
We have done everything possible to politicize medicine and science this year in this country – and look where it has gotten us. People not just here but all over Twitter and our media screaming at one another about things they have no clue about – just because their side says so. It has been a revelation.
I would also like to echo one of the above commenters – decrying the fact that most practicing physicians have just been cut loose to flap in the wind. Trust me – there are many days when I feel just like that. We have not had time for science in this pandemic to give us real answers – but the more unfortunate thing is that our national agencies have not even tried. The minute that these overwhelmingly positive studies were coming in from other countries about Ivermectin – our NIH and other agencies should have immediately been on the ball – working on our own rigorous studies. They have been nowhere. That has led physicians like me to use the drug despite our own credulity in the beginning (Lice pills? You have got to be kidding!) – guess what – it seems to be working to keep people out of the hospital. And it is not nearly as scary as the other option, monoclonal antibodies (MONOCLONAL ANTIBODIES, WTF?) to keep people out of the hospital. And I remind you – the monoclonal antibodies are on an EUA just like the vaccines – and are considered the same status as Ivermectin by the NIH. This is a safety no brainer – and yet my profession and our country seems hell bent on laughing off the 8 dollar a month safe 40 year experience pill for something that is equivalant to a dose of chemotherapy – with really no strong efficacy numbers to balance out the risk. And they are thousands of dollars a dose.
Our nation’s medical leadership has been all over the place this year – wear masks – don’t wear masks. 3 foot social distance – 6 foot social distance. You all know exactly what I am talking about. Instead of leadership, they have often gotten on national TV to fear monger and even cry like yesterday.
Meanwhile, there are thousands of physicians like myself in communities all over this country doing our best to hold it all together for our patients. Not just the COVID patients, the countless others who have lost jobs and livelihoods and lifelong businesses. We are seeing all kinds of vaccine complications – while the media and medical elites are screaming that they are 95% effective and perfectly safe. I am praying every day that the vaccines work – and it was worth the risk – the backlash if not will be unforgiving.
That is where I am today. I will continue to use ivermectin to keep people out of the hospital. It seems to be as effective as any other modality we have right now. I will keep my eyes peeled for studies and evidence about this issue. Antivirals are going to be as critical going forward as vaccines.
And for those questioning why doctors are remaining anonymous ( a trend that was never dreamed of during AIDS) – you really must be dense. Look at the cancel culture in which we live. We as a country need some serious introspection when good faith questioning leads to job loss and career suicide.
To Yves and Lambert – like everyone else – you are not 100% right all the time. The definition of humanity. But you have given thinking people a forum to discuss and learn. For that we should all be eternally grateful. You are doing a great service to our world.
“We are seeing all kinds of vaccine complications ”
Could you be specific? Maybe I missed prior posts of yours.
Also, just wanted to say “thanks” for your contributions.
Reactions by those with autoimmune diseases. Multiple reports from people who are one degree of separation removed from me of a significant worsening of symptoms after getting the Pfizer and Moderna vaccines, and that not abating over time.
Just an anecdote but good to know from someone with an autoimmune condition. I have been worried about this and can’t get any information from doctors or the internet. I figure I have to wait a year until the shit hits the fan (or not) to see what shakes out. So frustrating.
What am I seeing?
The most fascinating problem that has no obvious explanation is a surprisingly large number of patients that get sick and are COVID positive within hours/days of their first injection. I have heard all kinds of lame excuses why this may be happening – but none of them really ring true for the numbers that are occurring. I would predict this is going to be an interesting story when the full story of COVID comes out in a few years. By the way, they tend to be WAAAAY more sick than a regular COVID patient. No hospitalizations yet.
I am seeing blood clots in both venous and arterial systems. This is happening mainly to younger people. I have 4 so far – an unexpected DVT, a PE, a very strange problem in a young healthy man having unstable angina with positive enzymes within hours of his first shot, and a young woman who clotted off the main artery to her arm on the injection site leading to a compartment syndrome. None of these patients have died – and all are doing well now. But it was scary when it was happening. No proof the vaccines did it – but the timing is very concerning, especially in the last 2. I would reiterate that the PCPs of the world are flying blind in this regard. We have no guidebook of completed and well-done trials to guide us with what are common problems. We are literally just taking it all in as we go along. I will reiterate – in a decades long career – these things I have just outlined are 3 times as many severe complications as I have seen after giving 10s of thousands of other immunizations. This is the truth.
A handful of patients with sudden flares of their dormant autoimmune syndromes – one of which is turning into something possibly bad. Multiple patients with COVID negative and severe URI symptoms. And multiple severe issues with lymph nodes almost to the point of being bubos. I have also seen a severe Ramsay Hunt syndrome in an elderly woman and one episode of anaphylaxis.
That is all I can remember off the top of my head. Maybe these all have nothing to do whatsoever with the vaccines. The timing, however, is very suspicious. And please note – this is a handful of severe problems in probably 1500 to 2000 vaccinated already. The number of people with fever, chills, flu-like illnesses, etc has been very high, just as predicted in the protocols. But the vast majority of patients have no obvious long-term problems. It is my contention that the patients of the world should have had this presented to them correctly – and we would all be better off emotionally. But alas – it is what it is. Younger people seem to be having a much worse time with side effects – now that we are moving into the younger age groups, I fear this is going to become a much more significant issue.
> the patients of the world should have had this presented to them correctly – and we would all be better off emotionally.
It does seem that, at least at the top level of the public health establishment, lying to the public to achieve an acceptable outcome is considered best practice (see Fauci on masks). Those lying must not perceive the practice as maladaptive from a career perspective, so one shudders to think of the state of the institutions through which they rose.*
* “Everything is like CalPERS.”
Actually we have precedents for the observation you mention on cases cropping up early from other vaccine trials and we now have DATA from two vaccine studies for this vaccine that document what you are saying.
I adopted a rescue dog from coastal North Carolina in 2012 that had a bad case of heart worms. The universally accepted treatment is a dangerous (and very expensive) two-dose injection of arsenic to the dog’s spine followed by cruelly immobilizing the dog in a tiny crate for six weeks. The shots leave many dogs with permanent paralysis and many more die from blood clots formed by rotting masses of dead heart worms which die off suddenly from the injections. A small town Vet in North Carolina who was very skeptical of the cruel and high-risk injections tipped me off to a University of Georgia study where dogs were successfully cured of heart worms using a standard prophylactic dose of Ivermectin and intermittent Doxycycline. I ran the idea by my very caring, intelligent and open-minded Vet in Manhattan and after reading the study said he was willing to try the alternative treatment. The one-two punch of the Ivermectin and three-cent-a-pill Doxycycline worked like a charm and my dog was heart worm free after six months without being cruelly confined or running the risk of paralysis or sudden death. The vet was amazed and swore he would never recommend the standard heart worm treatment again. I saved myself about $3000 as well, and while the amount was significant to me, that was just icing on the top not the prime motivator for seeking an alternative treatment. However, for many pet owners, that sum could be the difference between seeking treatment and letting a dog slowly succumb to parasites. I researched the dangerous and expensive shot and why it was universally accepted in the United States as the only legitimate cure for heart worms and the answer seemed to be strategically placed board members among prestigious Veterinary Schools and a quite few lavish Marlin Fishing junkets funded by the pharmaceutical company producing the arsenic shot. Yes, veterinary medicine I know, but from what I’ve learned Veterinary medicine and Human medicine operate exactly the same in the US. Never treat anything with a pill that cost pennies if you can use a shot that costs thousands, even if the more expensive treatment paralyses and/or kills the patient – large profits are far more important to the functioning of the system than curing disease or minimizing harm. When it comes to medicine trust no-one receiving payment, do your homework and plan on advocating for yourself at every turn.
This story is heartwarming, but it’s no proof ivermectin is a good covid treatment.
It’s amazing how skeptical folks are of Big Pharma’s PR, but how incredulous they are for “heartfelt anecdotes.”
Never said my story was proof Ivermectin is a COVID miracle drug. Just a real world example of how Ivermectin has been dismissed as a treatment option by the (Veterinary) medical establishment due to a Capitalist preference for a more expensive, but less desirable treatment. Furthermore this isn’t a ‘heartfelt anecdote’ but a firsthand account. I think the treatment regime I detailed has gained a bit more acceptance for heartworms now, but it was virtually unheard of in 2012 despite published research showing efficaciousness dating back several years. The other parallel of my story is the economics and availability of the preferred medicine of western doctors in highly developed countries frequently mean nothing to those without the financial means to obtain the treatment, and in some countries the drugs simply aren’t available to people, necessitating alternative treatments and experimentation, which most I think most would agree is preferable to dying. I have no dog in this fight ( pardon the pun ) but I do have experience with Ivermectin being sold short as a drug by credentialed medical experts in the pursuit of profits.
*** crickets *** in response…
Reminds me of Doris Cully talking about ivermectin talking about river blindness and allowing time for clearing the parasite from the eye — about 14 minutes into the podcast. Sounds like the mass of dead worms you mention.
About 3 minutes in Doris Cully relates her background working with ivermectine when it was discovered.
forgot to give link https://www.microbe.tv/twiv/twiv-599/
Thank you for this and your other comments. I watch for and greatly value your insights and revelations offered through your view from the trenches of medical practice.
Before the Corona pandemic I had been growing pessimistic about how Humankind would respond to Global Warming and the impending limits to growth, and about what prospects the future held. After a year of the Corona pandemic observing the incompetence, greed, and cruelty of the US Government, and organizations, agencies, authorities, and disciplines that once held my highest regard, mishandling the pandemic and the ongoing economic disasters it created, my pessimism nears fatalism regarding prospects for the future of Humankind, myself, and my children.
A recent addition to the FLCCC website is a page “How To Get Ivermectin” offering a list of physicians who will prescribe ivermectin.
https://covid19criticalcare.com/guide-for-this-website/how-to-get-ivermectin/
Thank you very much for this valuable information.
I grew up stock farming in the great Ivermectin boom when every farmer was recommended to drench his cows (forced oral administration) with it against liver flukes and the like.
Ivermectin, IIRC, is notorious in the organic farming community for producing “plastic cowpats” – cowpats that do not degrade and support insect populations but dry into frisbees. The difference between organic cow manure and intensively farmed is profound.
So, if you do take it off-label, just be aware your microbome might need some serious restoration of your commensal bacteria and parasites. Low parasite loads are linked with many autoimmune diseases and gut disorders.
I still think the data on Ivermectin justify proper randomised clinical trials. The examples and counterexamples are just too noisy. Even the argument about effective concentration is not clear: in vitro is not in vivo because compounds exhibit preferences for different tissues (volume of compartmentation), which is why chloroquine reaches effective blood cell concentrations on low regular doses and, after many years, can lead to blindness because of the effects of high retinal concentration.
> I still think the data on Ivermectin justify proper randomised clinical trials.
They do indeed (though many of the RCTs for HQ seemed almost designed to produce a negative outcome, not being designed to test for prophylaxis).
However, given the givens, I think the threshold could be — is, obviously, already in many countries — lower than RCT. Zeynep Tufecki writes, of RCTs and masking:
So far as making public health decisions in a pandemic, I don’t see why the enornous natural experiments listed in the post aren’t enough to go forward on, RCT or no RCT.
To do it right, studies for all the possible drugs should be funded, and research funding, which is pitifully stingy, should have been ongoing for decades, including genomic research and such into possible vectors for zoonotic diseases, such as bats. This is a constant complaint among researchers (corona virus among deer mice, for one example I heard). We seem to be too preoccupied with finding new ways to blow ourselves up for that however.
Reality check from the CDC’s Mortality and Morbidity Weekly Report: “Among 148,494 U.S. adults with COVID-19, a nonlinear relationship was found between body mass index (BMI) and COVID-19 severity, with lowest risks at BMIs near the threshold between healthy weight and overweight in most instances, then increasing with higher BMI. Overweight and obesity were risk factors for invasive mechanical ventilation. Obesity was a risk factor for hospitalization and death, particularly among adults aged <65 years.”
Body Mass Index and Risk for COVID-19–Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death — United States, March–December 2020 | MMWR
https://www.cdc.gov/mmwr/volumes/70/wr/mm7010e4.htm?s_cid=mm7010e4_w
AKA: If you are already “ill” (Obese) it take less effort for disease to kill you.
That’s not a surprise.
I suspect there is a causal link between Obesity, Air Conditioning and Driving, as both air conditioning and driving appear to eliminate exercise appear to promote obesity (through lack of exercise) and its attendant ills.
I used the site AmericasFrontlineDoctors which takes you to speakwithanMD.com to get my 80 year old father ivermectin. After the consult, they sent him hydroxychloroquione/zinc instead, and they have not responded to any of my emails/texts inquiring if that was done due to possible interactions with my father’s other medications.
From my reading, and I’m not an MD or biomed person, I believe there are a few ivermectin contraindications – like pregnancy and liver disease – and drug interactions – like Warfarin and coumadin. Don’t take my word. This is one reason it’s so important to talk to your doctor about whether it’s an appropriate med for your medical condition.
It’s infuriating the US pharma/med/govt nexus is trying to stop your local MD who knows your med history from prescribing ivermectin when appropriate.
> I used the site AmericasFrontlineDoctors which takes you to speakwithanMD.com to get my 80 year old father ivermectin. After the consult, they sent him hydroxychloroquione/zinc instead, and they have not responded to any of my emails/texts inquiring if that was done due to possible interactions with my father’s other medications.
Well, so much for them! (One of the disadvantages of being an outsider is lack of resources, and one of the dangers is zealotry.)
So why do you trust “America’s Frontline Doctors” over Big Pharma?
Or is this organization NOT selling you something?
As alternative treatments always do, this reeks of “we care, not like horrible Big Pharma!”
Great bedside manner is the entire foundation of a quack’s practice. A great mild example is Cancer Treatment Centers of America. Expensive, but they support you with alternative treatments! And there survival rates look great! Must work, right?
They get those rates by not admitting folks with low survival probabilities. It’s much money for a kinder, more pleasant environment. Which feels “healing.”
“Well, it can’t hurt..”
Sorry, TANSTAAFL applies. The cost may be low, but there is a cost. Quackery crowds out resources for real treatments.
Ignoring the actual evidence in the post entirely. But you do you.
TANSTAAFL is Libertarian code speak for Neo-liberal Rule #2.
(Here we go again!)
Update: Yay! It worked! I have no clue as to why the previous comments were eaten by the Internet Dragons. Oh well. Perhaps the “gods” are trying to teach me something about the quantum nature of reality.
Since there is now an article dedicated to this subject, here is a related link from an MD who specializes in bioweapons: https://anthraxvaccine.blogspot.com/2021/01/first-country-bans-ivermectin-lifesaver.html
She first came to my attention after the anthrax mailing scare years ago as a skeptic against the official narrative. I thought of her again when Covid started and I’ve been reluctant to post anything from her here before, since she is once again going against the official narrative. I have no idea how she is regarded within her field, she does get tend to hyperbole a bit in the link above, and I don’t know nearly enough about medicine to evaluate what she says in this and other posts of hers I’ve seen across the interwebs over the last year. That being said, while I’m not a regular follower of her blog, I have checked in over the years when microbes are in the news and she does seem to have a lot of knowledge in her field and comes across as a genuinely decent human being. Also, she is from Maine!
Her other writings on the coronavirus topic, including what I thought was decent argument debunking a study claiming chloroquine was not only ineffective but dangerous (she said it is dangerous when they drastically overdose people like they did in the study, but not when used in proper dosages) can be found with a quick search for anyone interested. Or you can just read more on her blog linked to above, but the blog may not have the most detailed and scientific arguments compared to other writings.
I would be genuinely interested in what others with a better understanding of virology/vaccines make of her take.
Of so many tragedies to come out of the COVID-19 pandemic, one of the saddest to me – and probably the one with the longest-reverberating consequences – has been its wholesale discrediting of our health science institutions.
Here we are, over a year into this pandemic, and we cannot get a straight answer on whether or not this relatively cheap and safe drug saves human lives from COVID-19 or not. Worse, we can’t even seem to properly investigate it. All questions bring hysterics, or hardly-believable obfuscation, or (informed?) outrage, no matter what authority we turn to. The fallout in my own life from watching all this unfold has been… dramatic.
I don’t trust what the CDC says. I don’t trust what the WHO says. I don’t trust what the FDA says. I don’t trust Pfizer and the rest of the pharmaceutical companies any farther than I can throw them. I look with suspicion on my own scientist acquaintances, wondering if they are really following the data, or if they are clinging to a chosen worldview that science in America still works, oh god it still works, oh god it hasn’t been completely discredited, no it cannot be, my life work must have meant something, it must still work, it must still work….??
None of this means that ivermectin works–or for that matter, that it doesn’t work. It means that I have realized, slowly and then all-of-a-sudden, that I cannot know. Nor can any other layperson. We are alone, our economy is collapsing in slow-motion, and our lives are at stake. Or so we think! If we doubt so much, how much more should we really be doubting? I believe, for what it’s worth, that COVID-19 is real and that these experimental vaccines probably won’t kill us. At least… not that many of us.
But I wonder now, in my darker moments, whether the claim of those who don’t believe such things that refusing the vaccination is a “Darwin’s test – pass it and survive” have grokked something that was beyond me, in my previous worldview. How could it have come to this…? And if I am feeling like this, how must people with less scientific background (I attended a science magnet school) be feeling about it all??
Will my children be safe from measles, etc in the years to come? I have vaccinated them with the whole slate, and feel fine about that choice, but will the fallout from this debacle mean the end of herd immunity in America, as trust in the ‘health experts’ collapses into dust? How can we get it back, then – at gunpoint? With all that would imply… is it even worth such a high price…?
NC is doing the Lord’s work in finding the high quality news sources it continually brings forth for our viewing. But – pardon me – this isn’t something that should need to be be argued over in the comments section of a news site. This isn’t something that laypeople should have to suss out, with their own lives on the line. That it has come to this is a shame, and a shame so complete, that every time I really contemplate it I get the shivers. Our government has failed us. It has failed us. Yet we elected it. Oh, the shame…!
Is it my fate to live the rest of my life ashamed, utterly ashamed, of my own country? There has been no feeling reoccurring more regularly over the course of this past dreadful year, than that one. When, if ever, will the day come where I can live free of that dreadful emotion, attacking me every time now when I catch a glimpse of that flag flapping in the wind…?
I could not have expressed many of my same feelings better. Thank you. And I am a medical professional. You should not feel alone in the chaos. Anyone who has a brain and the ability to reason has felt the same way all year.
My feelings echo your despair.
> Is it my fate to live the rest of my life ashamed, utterly ashamed, of my own country? There has been no feeling reoccurring more regularly over the course of this past dreadful year, than that one.
I have had the same feeling all this year, too.
My first comment from a long time reader. This heartfelt comment is exactly what has concerned me throughout this year. I thank you for so eloquently speaking what I consider truth.
Here’s another “Amen” from a healthcare person who is feeling dazed and confused by this year and is having a bit of an epistemological crisis — I feel much the same about the organizations you referred to.
As for the original post, I could hardly believe the vehemence of the reaction against hydroxychloroquine last year, since in my experience it’s not known to be overly dangerous. But I thought, “Ok, well, Trump Derangement Sydrome, Plus, it’s probably bad news to give it to someone really old who’s critically ill and
has a bunch of electrolyte disturbances etc..”
Now the pushback against Ivermectin. I have to wonder where it comes from. Who knew there was such widespread simmering emotion about a drug that most wealthy Westerners never encounter in their lifetime!
I don’t know. I’m probably just internet-poisoned but this whole thing stinks and now my question-everything paranoia directly affects my work life, so now I can’t get away from it. Argh!
I am so glad I am not having to administer the AZ vaccine yet! I’m supposed to be able to give patients an intelligent recommendation on these things, but I mostly feel like an idiot.
You have captured the essence of the New American Experience.
It feels like what someone losing a life long religious conviction must experience.
Are we going to have a “Lost Generation” like the West did after World War One?